
Biomedical Applications of Titanium Alloys: A Comprehensive Review

1
Ceramic Physics Laboratory, Kyoto Institute of Technology, Sakyo-ku, Kyoto 606-8585, Japan
2
Department of Dental Medicine, Graduate School of Medical Science, Kyoto Prefectural University of Medicine, Kamigyo-ku, Kyoto 602-8566, Japan
3
Department Polytechnic of Engineering and Architecture, University of Udine, 33100 Udine, Italy
4
Biomedical Research Center, Kyoto Institute of Technology, Sakyo-ku, Kyoto 606-8585, Japan
*
Authors to whom correspondence should be addressed.
Materials 2024, 17(1), 114; https://doi.org/10.3390/ma17010114
Submission received: 24 November 2023
/
Revised: 15 December 2023
/
Accepted: 21 December 2023
/
Published: 25 December 2023
(This article belongs to the Section Biomaterials)
Abstract
:Titanium alloys have emerged as the most successful metallic material to ever be applied in the field of biomedical engineering. This comprehensive review covers the history of titanium in medicine, the properties of titanium and its alloys, the production technologies used to produce biomedical implants, and the most common uses for titanium and its alloys, ranging from orthopedic implants to dental prosthetics and cardiovascular devices. At the core of this success lies the combination of machinability, mechanical strength, biocompatibility, and corrosion resistance. This unique combination of useful traits has positioned titanium alloys as an indispensable material for biomedical engineering applications, enabling safer, more durable, and more efficient treatments for patients affected by various kinds of pathologies. This review takes an in-depth journey into the inherent properties that define titanium alloys and which of them are advantageous for biomedical use. It explores their production techniques and the fabrication methodologies that are utilized to machine them into their final shape. The biomedical applications of titanium alloys are then categorized and described in detail, focusing on which specific advantages titanium alloys are present when compared to other materials. This review not only captures the current state of the art, but also explores the future possibilities and limitations of titanium alloys applied in the biomedical field.
1. Introduction
In recent decades, the intersection of materials science and biomedical engineering has yielded remarkable advancements in biomedical engineering. At the forefront of this convergence stands titanium, an elemental metal that, when properly alloyed, has proven itself to be a game-changing biomaterial [1]. Renowned for its unique blend of mechanical strength [2], biocompatibility [3], corrosion resistance [4], and the ability to promote integrative tissue interactions [5], titanium alloys have emerged as the most successful material in biomedical applications, in particular in the fields of orthopedics and dentistry [6].
The present comprehensive review tries to navigate the intricate landscape of titanium alloys’ biomedical applications—a journey that traverses numerous medical disciplines, from orthopedics [7] to dentistry [8] and even cardiovascular care [9]. With an emphasis on elucidating the core attributes that underpin their exceptional versatility, we delve into the mechanisms that are responsible for the success of titanium alloys, but also the limitations.
The story of titanium alloys’ foray into the medical world is closely intertwined with the groundbreaking work of Dr. Per-Ingvar Brånemark [10,11,12]. His pioneering research on osseointegration—a term he coined to describe the direct structural and functional connection between living bone and the surface of an implant—ushered in a new era of medical possibilities. The realization that titanium could serve as a “scaffold” to support—if not stimulate—bone tissue adhesion, growth, and integration led to a revolution in orthopedic and dental implantology. The impact of Brånemark’s contributions continues to reverberate, as his insights laid the foundation for the use of titanium and its alloys in modern medical applications and, in the last decades, no other structural metal was ever able to achieve the combination of performances shown by titanium.
In orthopedics, titanium is the most common choice for components that undergo heavy, cyclic mechanical solicitation, in particular for stems and cups in articulations such as shoulder, hip, knee, and ankle, for which polymeric materials would not reach the necessary strength. Apart from strength, titanium implants provide good secondary fixation as they undergo osteointegration over time [13], and the process can be further accelerated using cellular solid morphologies [14]. On the other hand, despite the scientific interest and the numerous attempted solutions [15], titanium has been shown to be unsuitable for components subjected to wear, such as in the case of femoral heads [16] in hip arthroplasty or femoral components [17] in knee arthroplasty.
In the field of dentistry, titanium has found application for dental posts, screws, abutments, braces, instruments, and also temporary devices. Compared to orthopedics, devices used in dentistry and orthodontics are under lower mechanical solicitations, but the oral cavity is a much harsher environment from the chemical and biological point of view. Constant changes in pH [18], release of aggressive chemical species from foods and beverages [19], presence of tartar/plaque [20], and proliferation of pathogens such as bacteria [21] can drastically reduce the chances of clinical success and the expected life span of biomaterials. In most cases, the chemical inertness of titanium has proven to be up to the task, but concerns are periodically raised about the potential release of harmful alloying elements [22], and allergic reactions have also been reported, in particular for titanium–nickel alloys [23].
Like orthopedics appliances, trauma devices such as screws, plates, and intramedullary nails are also subjected to intense solicitations, to the point that it is not unusual for surgeons to prefer the more resistant stainless steel over titanium [24]. Moreover, unlike most components used in arthroplasty, trauma devices are often removed after the healing process has been completed [25,26], and a perfectly osseointegrated titanium device would prove difficult to remove without damaging the surrounding tissue [27,28].
Despite spinal devices being technically a subset of orthopedic implants, they possess unique characteristics and, for the scope of this review, will be considered a separate category. Spinal implants that can make use of titanium or titanium alloys are pedicle screws, rods, inter-body cages, artificial discs, and all the hooks and wires that are used in the correction of spinal deformities such as scoliosis, so depending on the application, the device can be articulating (artificial discs) or locking (inter-body cages) bones into position, behaving either like an arthroprosthetic or a trauma device. Despite being, in most cases, subject to relatively low mechanical stresses, spinal implants face complex anatomy [29] with a great degree of variability among patients and can cause damage to the nearby nerves [30] and blood vessels and breakage is the most common type of failure in devices such as pedicle screws [31]. Moreover, the stiffness of titanium can delay the healing processes [32] or even cause unexpected bone fractures.
While titanium alloys’ preeminence in the field of orthopedics and dentistry has long been established, the combination of mechanical strength and biocompatibility promoted the use of titanium and titanium alloys in other fields of medicine, such as in cardiovascular devices. Titanium can be used as the main component of stents, heart valves, and vascular grafts, as well as parts of implantable defibrillators, pacemaker cases, and implantable sensors. Apart from biocompatibility, the most important requisite for cardiovascular implants is to be reliable over time, meaning that they are supposed to function without revision for long time spans. The revision of cardiovascular implants carries additional risks and, unlike most arthroprosthetic or dental devices, the mechanical malfunction of a cardiovascular device is life-threatening [33].
The main contents of this review, as well as the titles of sections and sub-sections, are summarized in Figure 1.
2. Properties of Titanium
Titanium is a chemical element with the symbol “Ti” and atomic number 22, nowadays recognized for its unique qualities that find practical use in various industries, from aerospace to automotive, military, sports, and even jewelry.
2.1. Physical Properties
Titanium undergoes a phase transformation from a hexagonal close-packed (HCP) crystal structure to a body-centered cubic (BCC) structure as a function of temperature. At room temperature, commercially pure titanium primarily exists in the α-phase, which has an HCP arrangement. As the temperature rises above approximately 883 °C (1621 °F), it transforms into the β-phase, characterized by the BCC arrangement [34]. This phase transition has an impact on various properties of the material, such as ductility and strength.
Titanium has a relatively low density of around 4.5 g/cm³, which is approximately half the density of steel or cobalt alloys. This low density contributes to its lightweight nature, making it highly desirable for applications where weight reduction is essential, such as in aerospace and medical implants. The low density is a key factor in reducing the overall load and movement inertia on the human body when titanium implants are used.
Titanium exhibits favorable thermal properties [35], including a high melting point of approximately 1668 °C (3034 °F). This high melting point enables the material to withstand elevated temperatures during manufacturing processes without losing its structural integrity. Additionally, titanium has a low thermal expansion coefficient, which means it expands and contracts minimally when subjected to temperature changes. This property is advantageous for applications where dimensional stability is crucial, such as in precision medical devices.
Titanium is a relatively poor conductor of electricity compared to materials like copper or aluminum, making it useful for applications where electrical insulation is desired [35]. In certain medical applications, such as implantable medical devices, the low electrical conductivity of titanium can be advantageous to prevent unwanted electrical interactions with the body’s tissues.
2.2. Chemical Properties
Thanks to its affinity towards oxygen, when exposed to oxidizing environments titanium spontaneously forms a superficial layer of protective oxide. This oxide layer is essential for the corrosion resistance of titanium and plays a crucial role in its biocompatibility and other applications, in particular at high temperature. Titanium oxide has two different crystalline forms, anatase and rutile, and their formation depends on the environmental conditions. Similarly, the thickness of the native oxide layer on titanium can vary depending on factors such as exposure conditions and the specific alloy composition, generally ranging from a few nanometers to about 10–30, and alloys exposed to humid air at room temperature have shown to form prevalently composite layers of titanium (IV), titanium (III), and titanium (II) oxides [36].
In biomedical applications, the presence of the native oxide layers plays a crucial role in biocompatibility [37], as it forms a barrier between the biological environment and the “reactive” metal underneath. The layer acts as a protection both against corrosion, as the biological environment is particularly aggressive towards metals, and against adverse reactions such as severe inflammations.
2.3. Mechanical Properties
Titanium alloys exhibit impressive mechanical strength and stiffness, providing the required load-bearing capacity for applications like orthopedic implants and dental prosthetics. The specific mechanical properties can be tailored by alloying with other elements, with some alloys reaching ultimate loads comparable with those of technical steels. Like steels, titanium alloys possess a fatigue limit [38] and display excellent fatigue resistance [39], making them suitable for long-term use in dynamic environments, such as orthopedic implants subjected to cyclic loading. Moreover, titanium alloys have a relatively low modulus of elasticity compared to other metallic materials applied in the biomedical field, which helps reduce the stress shielding effect, minimizing the loss of bone density around implants.
2.4. Biological Properties
Despite acting as a physical barrier between the metal and the biological environment, the native layer of titanium oxide formed on the surface of titanium and its alloys is not completely inert. As observed by Dr. Brånemark, bone tissue can adhere and grow on the surface of titanium alloys, to the point that titanium-based devices can be completely osseointegrated over time [40,41,42]. Titanium’s ability to integrate with bone, known as a key biomedical property, and various types of biomedical devices, such as scaffolds, makes use of this property to accelerate bone tissue regeneration or to improve adhesion and stabilization. Another property associated with the presence of native oxides is that titanium is considered hypoallergenic, as it rarely triggers allergic reactions in patients. This is especially important for medical devices in prolonged contact with the body. Moreover, titanium and its alloys are generally considered non-toxic and they supposedly do not release harmful substances into the body, ensuring patient safety over extended periods. Some concerns have been raised on the potential toxicity of a few, specific alloys, such as titanium grade 5 [43] or Nitinol [44], due to the presence of aluminum/vanadium and nickel, respectively.
3. Fabrication Techniques
3.1. Production of Pure Titanium
Titanium is primarily produced using methods that are specific to its unique characteristics. The two historically more relevant processes for producing commercially pure titanium are the Kroll process and the Hunter process:
Kroll Process [45]: The Kroll process is a primary method for producing titanium metal from its ores. In this process, titanium tetrachloride (TiCl4) is obtained by reacting titanium ores (typically ilmenite) with chlorine gas. The TiCl4 is then reduced to metallic titanium using magnesium metal in a high-temperature reactor. The reaction forms magnesium chloride as a byproduct. The process involves multiple stages, including chlorination of the ore, condensation of TiCl4, reduction of TiCl4 by magnesium, and separation of titanium sponge from magnesium chloride. The produced titanium sponge contains impurities and must undergo further processing steps to purify and refine the metal. Despite its complexity, the Kroll process remains a fundamental method for industrial titanium production, especially for aerospace, medical, and industrial applications.
Hunter Process [46]: The Hunter process is an alternative method for producing titanium metal from its ores. In this process, titanium tetrachloride (TiCl4) is also obtained by chlorination of titanium ores like ilmenite. However, instead of using magnesium for reduction, the Hunter process employs sodium or a sodium–potassium alloy as the reducing agent. The reduction takes place at a lower temperature compared to the Kroll process. A sodium or sodium–potassium alloy reduces TiCl4 to form metallic titanium and sodium or potassium chloride as byproducts. The resulting titanium sponge is then processed further to remove impurities and refine the metal. The Hunter process offers advantages like lower operating temperatures and reduced energy consumption compared to the Kroll process. However, it is less commonly used in industrial titanium production.
3.2. Production of Titanium Alloys
To produce titanium alloys starting from commercially pure titanium, particular care has to be given to the prevention of oxidation. For this reason, only a few technologies are commonly used:
Vacuum Arc Remelting (VAR) [47]: VAR is a commonly used technique for melting and refining titanium alloys. It involves melting a consumable electrode under vacuum conditions using an electric arc. This process helps to reduce impurities and control the alloy’s composition.
Plasma Arc Melting (PAM) [48]: PAM is another vacuum-based melting technique that employs a high-energy plasma arc to melt the material. It offers better control over composition and is suitable for producing specialty alloys.
Induction Melting [49]: Induction melting is used to produce small quantities of titanium alloys. It involves using electromagnetic induction to melt the material within a crucible in a controlled atmosphere.
Powder Metallurgy [50]: Powder metallurgy is mainly used as a near-shape production technique for titanium components, but by mixing powders with different chemical compositions, it is possible to use it as an alloying technique as well.
It is important to note that these production techniques are specialized and require stringent process control due to titanium’s reactivity and sensitivity to impurities. The choice of production method depends on factors such as the desired alloy composition, the quantity of material needed, and the specific properties required for the end application.
The formation of the undesirable alpha case [51], a hard and brittle layer of alpha-phase titanium, poses challenges during production processes involving high temperatures and reactive environments [52]. The alpha case can weaken mechanical properties [51] and induce implant failure. To counteract this, careful control of processing parameters and the utilization of protective environments are essential.
Moreover, the biocompatibility of titanium alloys depends on element concentrations. Elements such as aluminum and vanadium in excess can trigger toxic effects, thus stringent controls on composition are necessary [53,54,55]. For instance, Grade 5 titanium (Ti-6Al-4V) used in orthopedic implants and dental prosthetics, requires careful alloying to avoid cytotoxicity.
4. Titanium Alloys
4.1. Main Microstructural Phases
Most titanium utilized for the production of biomedical devices is alloyed with other elements, and even the commercially pure titanium grades actually contain small amounts of trace elements that have a clear influence on their final properties.
As discussed in Section 2, titanium alloys exhibit mainly two primary crystalline structures: alpha (α) and beta (β), where the α-phase has a hexagonal close-packed structure and the β-phase a body-centered cubic (BCC) structure. The partition between these phases significantly influences the material’s mechanical properties. Pure titanium has a transition temperature, known as the beta transus temperature, above which it transforms from the α-phase to the β-phase, but the transformation is reversible so commercially pure titanium grades do not have stable residual β-phase when they are cooled down from temperatures above the beta transus. Before discussing the effects of the alloying elements on the stability of the α- and β-phases, it is important to consider that titanium alloys, as basically all other metals, can also form several both stable and metastable phases. A comprehensive list of titanium alloy phases, along with their symbols and space groups, is listed in Table 1.
4.2. Effects of the Alloying Elements
Alloying elements play a pivotal role in tailoring the properties of titanium alloys. Traditionally, titanium-alloying elements are divided into two groups, depending on the phase they tend to stabilize. Alloying with elements like aluminum, tin, and zirconium stabilizes the α-phase, enhancing strength and hardness, and increasing the beta transition temperature [62]. Elements like molybdenum, tungsten, chromium, iron, silicon, and copper stabilize the β-phase, improving ductility and high-temperature performances, and also decreasing the beta transus temperature [56]. Vanadium and niobium can act as an α- or β-stabilizer, depending on the composition of the alloy [63]. Additionally, light elements such as oxygen and nitrogen also have an α-stabilizing effect and a neutral effect on beta transus temperature. The role of alpha and beta stabilizers in the control of the microstructure of titanium alloys is summarized in Figure 2.
The combination of these alloying elements allows for the creation of alloys with a wide range of mechanical properties, biocompatibility, and corrosion resistance. Conventionally, titanium alloys are divided into five categories, depending on their chemical composition and expected microstructure in service. The five categories are:
Alpha Alloys [62]: Primarily α-phase structures. This category comprises both unalloyed titanium and alloys containing α-stabilizers, such as aluminum and tin that are prevalently used for aerospace applications (Figure 2c).
Near Alpha Alloys [64]: Predominantly α-phase with limited β-stabilizers. Balance of strength and formability.
Alpha-Beta Alloys [65]: Balance of α- and β-phases, offering a combination of strength, ductility, and heat resistance, commonly used in a wide range of applications (Figure 2d).
Near Beta Alloys (or Beta metastable) [66]: Predominantly β-phases with limited α-stabilizers. When compared to α-β alloys, they sacrifice mechanical strength to improve the ductility.
Beta Alloys [67]: Predominantly β-phase alloys with elements like vanadium and molybdenum.
There is another titanium-based structure that is technically considered to be a nickel–titanium intermetallic. For the sake of this review, Nitinol will be considered a titanium alloy, despite containing about 55% nickel. This choice is mainly due to the large number of important biomedical applications and its availability on the market [68]. This material has been added to complete the panorama of Ti-based alloys used in biomedical applications. However, being an intermetallic and not technically an alloy, it will not be discussed in further detail in this review.
4.3. Biomedical Titanium Alloys
The main alloys applied in the biomedical field, along with their microstructures and applications, are listed in Table 2, while the relationship between their elastic modulus and their ultimate strength is presented in Figure 3.
Despite the wide range of possible alloys, commercially pure titanium grade 2 and Ti-6Al-4V grade 5 are used in more than 95% of all titanium biomedical devices. Also widely used in the biomedical field are ELI (Extra-Low Interstitials) alloys, whose main chemical composition is similar to that of the above alloys, but with very low levels of interstitial elements. A reduction in the levels of interstitial elements (O, N, H, and B) in the alloy has a beneficial effect in increasing the ductility and fracture toughness of the material [118].
4.4. Effects of Heat Treatments
Like all other alloys, heat treatments can be utilized to control the microstructure and properties of titanium alloys, but the low thermal conduction of titanium makes microstructure control more challenging when compared to other high-performance alloys such as steel. The lack of microstructural control is more evident in thick components where the differences in cooling rates between the core and surface are affected by the above property.
Another important weakness in the heat treatment of Ti alloys is their reactivity with many gases such as O and N, which tend to promote the formation of the detrimental alpha case layer on the outer surface. To avoid this problem, heat treatments are usually carried out under vacuum and the fast-cooling rates are usually achieved by gas cooling with inert gases. This also highlights that the Ti alloys are sensitive to cooling rates during quenching [119,120].
No strengthening heat treatment can be performed on α- and α-near titanium alloys. Both types of alloys can be stress-relieved and annealed (also recrystallization treatment), but high strength cannot be developed in these alloys by any type of heat treatment, as the alloy consists of only one stable phase.
In the case of commercially pure titanium, the trace elements play a critical role in the mechanical performance, and both Oxygen [121] and Iron [122] contents are usually close to the maximum allowed amount to increase the strength of the material. Usually, the O content is lowered to increase the toughness of the material [123].
- Stress-relieving: Mainly utilized to reduce undesirable residual stresses that may result during material processing, usually performed at temperatures between 595 and 705 °C (1100 and 1300 °F) for a period of one to two hours, for alpha and Alpha–Beta alloys, and at 700–800 °C with shorter times, for beta alloys. Cooling is usually performed in air. Stress relieving does not alter the overall microstructure or phase distribution. The main effect is to improve the material’s mechanical properties that are sensitive to residual stresses (e.g., fatigue).
- Annealing: Annealing titanium and its alloys primarily aims to enhance fracture toughness, room temperature ductility, dimensional and thermal stability, as well as creep resistance. As it maximizes some of the most important technological properties, many titanium alloys are placed in service in their annealed state. There are two common types of annealing for titanium alloys that are relevant for biomedical applications, and the most suitable treatment depends on both the chemical composition and the scope:
- −
- Recrystallization annealing: By heating the alloy up to the upper end of the α-β range (but still below the β-transus), recrystallization annealing helps refine the grain structure of titanium alloys. It promotes the formation of new, smaller grains with a lower dislocation density, which enhances mechanical properties such as strength and ductility. It also contributes to eliminating cold work effects and residual stresses.
- −
- β-annealing: It involves heating the material within the beta-phase region (but usually as close as possible to the β-transus) to enhance its mechanical properties. Held at a specific temperature range, this treatment facilitates the dissolution of unwanted phases, reduces residual stresses, and promotes the formation of a uniform microstructure.
- −
- Duplex annealing: Duplex annealing of titanium alloys entails a two-step process. The alloy is initially heated to the beta-phase region for homogenization, eliminating chemical inhomogeneities. Subsequently, a second annealing in the alpha-beta region refines the microstructure, improves mechanical properties, and minimizes residual stresses. Duplex annealing is commonly applied to α-β titanium alloys, particularly those used in aerospace and high-performance applications.
- Solution treating and aging: In solution treating, the alloy is heated to a high temperature within the beta-phase range to dissolve alloying elements and achieve a homogeneous solid solution. Rapid quenching locks in this solid solution. Aging, the second step, involves reheating the alloy to a lower temperature to encourage precipitation of fine particles. These particles contribute to strengthening and refining the microstructure. The balance between the alpha and beta phases, achieved through proper aging, enhances mechanical properties, such as strength, hardness, and fatigue resistance. The specific temperatures and times for these processes depend on the alloy’s composition and intended application.
Biomedical titanium alloys make use of most of these heat treatments, depending on the production technique, the chemical composition, and the intended application. Forged components, such as femoral stems, usually require a stress-relieving treatment before they can be machined and finished. Nitinol, on the other hand, is usually annealed at high temperature to dissolve precipitates and impurities.
5. Forming of Titanium Alloys
Ti alloys can be purchased conventionally as cast or after some plastic deformation (hot or cold working) to shape the component and control the microstructure. The melting process is usually carried out by induction or arc melting under a protective atmosphere to avoid oxidation of the molten bath. The highest quality molten baths are obtained using vacuum processes (VIM or VAR). The material is then cast in water-cooled copper molds to produce ingots, which are then machined to their final shape. Cast materials are not only used for components with complex shapes, such as femoral stems [127,128], but also on more simple devices such as titanium posts for dental applications [129,130,131]. In this case, the liquid metal processed by the above techniques is poured into a mold with a geometry close to the final shape of the component and then sometimes centrifuged to improve uniformity and mechanical properties [132]. The microstructure of the material is related to the solidification conditions and the alloy content.
Ti-alloys can also be formed by intense plastic deformation at high temperatures [133,134,135]. The raw material is usually a sheet or preformed material. Conventional forming consists of forging the material at temperatures in the range of 800–1000 °C. In this case, during the forming process, the most important parameters for forging the material are temperature and strain rate. It is important to limit the gas interaction of the forged material in order to avoid the formation of an alpha case layer. On the other hand, the stamping process is often used to obtain components produced by deforming the material at warm temperatures (300–400 °C) by sheet deformation. By increasing the temperatures and controlling the strain rates, it is also possible to reach a superplastic regime, which is useful for the production of very complex shapes where triaxial deformation is required. Most of the emerging techniques in the biomedical field are related to severe plastic deformation, which results in a material with a significant increase in mechanical properties due to the severe grain refinement that the material undergoes. These processes are equal channel extrusion [136], accumulative roll bonding [137], multidirectional forging [138], and twinning extrusion [139]. The process temperature to obtain a micrograin structure is in the range of 400–600 °C.
6. Machining of Titanium Alloys
6.1. Conventional Machining
The production of biomedical titanium components involves a range of techniques tailored to meet specific application requirements. For orthopedic and dental implants, the most common production method is precision machining [140], which offers precise geometric control and surface finish. However, machining can introduce residual stresses and potential surface damage, affecting mechanical integrity and implant performance [141,142]. Thus, post-machining treatments are crucial to relieve stresses and restore material properties.
In more complex cases, for example for the production of cellular solids such as scaffolds for tissue regeneration, additive manufacturing (3D printing) has gained prominence, enabling the creation of complex, patient-specific implants with porous structures to promote osseointegration. The effects of 3D printing on the microstructure [143,144,145] and the consequent post-processing treatments [146,147] will be discussed in the next chapter.
Machining titanium alloys can be challenging due to their excellent combination of strength, low thermal conductivity, and chemical reactivity. However, several machining techniques are employed to shape and finish titanium alloy components for various applications. In addition to conventional machining techniques like turning, milling, drilling, and grinding, titanium is frequently processed using more advanced technological methods, such as electrical discharge machining, abrasive water jet cutting, laser machining, and ultrasonic machining. Given that these techniques are less common, a brief description of each is provided in the next paragraph, to benefit the reader.
6.2. Advanced Machining
Electrical Discharge Machining (EDM) [148,149]: Electrical Discharge Machining (EDM) is an advanced metal removal process used to shape intricate and complex geometries in titanium alloys and other materials that are electrically conductive. In the context of titanium alloys, EDM offers a unique advantage due to their inherent hardness and challenging machinability. In EDM, a precisely controlled electrical discharge, or spark, is generated between a tool electrode and the workpiece submerged in dielectric fluid. This controlled spark erosion method selectively removes material from the workpiece without direct physical contact. The dielectric fluid acts as a coolant and insulator, flushing away the eroded particles. For titanium alloys, which possess high melting points and low thermal conductivity, EDM is particularly useful. The process can achieve precision cuts without inducing thermal damage or distortion, which is common with traditional machining methods. EDM is well suited for intricate shapes, thin sections, and hardened surfaces, which are characteristic of titanium components used in aerospace, medical implants, and more. However, EDM does have limitations in terms of material removal rates and surface finish. The process is generally slower compared to traditional machining methods, and a post-EDM finishing step might be required to achieve the desired surface quality. Despite these limitations, EDM remains a valuable technique for titanium alloys due to its ability to work with hard and intricate materials, where conventional methods often fall short.
Abrasive Water Jet Machining (AWJM) [150,151]: AWJM is a material removal process that is particularly advantageous for shaping and cutting titanium alloys and other hard-to-machine materials. Titanium alloys, with their high strength and resistance to heat, often benefit from the capabilities of AWJM. In this process, a high-velocity stream of water mixed with abrasive particles is directed towards the workpiece. The abrasive particles, often garnet or aluminum oxide, effectively erode the material due to their high kinetic energy. The controlled mixing of water and abrasive allows for precise material removal, and the process can accommodate a wide range of thicknesses and complexities. For titanium alloys, AWJM offers several benefits. Its non-thermal nature prevents the risk of heat-induced distortion or damage, which can be a concern when using traditional machining methods. Additionally, the absence of mechanical stresses associated with conventional cutting minimizes the risk of work hardening, which is common in titanium. AWJM is suitable for intricate shapes, stacked material layers, and composite structures present in titanium components used in aerospace, automotive, and medical applications. However, achieving a smooth surface finish might require secondary finishing processes, as AWJM can produce a slightly rough surface due to the abrasive action.
Laser Machining (LM) [152,153]: LM is a manufacturing process that holds significant promise for shaping and engraving challenging materials. For titanium alloys, LM has garnered attention due to its ability to overcome the difficulties associated with their high strength and heat resistance. In LM, a high-energy laser beam is focused onto the workpiece, where it melts, vaporizes, or ablates the material. The precision and intensity of the laser can be finely controlled to achieve intricate cuts, fine details, and complex shapes. Titanium alloys, with their ability to absorb laser energy effectively, make them suitable candidates for this technique. LM offers multiple benefits. Its non-contact nature eliminates tool wear, reduces mechanical stresses, and minimizes the risk of introducing impurities into the material. Additionally, the localized heat input minimizes the heat-affected zone, reducing the potential for distortion or residual stress. LM is well suited for aerospace, medical, and automotive applications where precision and minimal material loss are critical. However, achieving optimal results might require adjustments to laser parameters based on the alloy’s composition and thickness. Despite the clear advantages, LM may generate an undesirable surface roughness, necessitating post-processing steps to achieve the desired finish.
Ultrasonic Machining (UM) [154,155]: UM is a material removal method that offers unique advantages for shaping and machining hard materials. In the case of titanium alloys, UM addresses the challenges posed by their high hardness and toughness. UM involves the use of ultrasonic vibrations, typically in the range of 20 to 40 kHz, to facilitate the removal of material from the workpiece. A tool, often made of softer material than the workpiece, is pressed against the workpiece while ultrasonic vibrations are applied. The abrasive slurry consisting of abrasive particles suspended in a liquid helps in the material removal process. The non-thermal nature of the process prevents the introduction of heat-induced distortion or changes in the material’s properties. Overall, UM is suitable for applications where traditional machining techniques might struggle, such as aerospace components and medical implants. However, it might require longer machining times compared to conventional methods, and, as seen for other advanced machining techniques before, post-processing might be necessary to achieve the desired surface finish.
Machining titanium alloys requires careful consideration of cutting parameters, tool materials, tool geometries, and cooling/lubrication strategies to manage heat generation and tool wear [156]. The reactivity of titanium with cutting tool materials can lead to chemical reactions and wear, necessitating the use of suitable tool coatings. Additionally, proper chip control and effective removal of heat from the cutting zone are critical to ensure dimensional accuracy and surface quality. Moreover, the heat generated at the tool-workpiece interface can cause localized temperatures to rise. In the presence of oxygen, this elevated temperature can lead to the diffusion of oxygen into the titanium, causing, as discussed before, the formation of a thin layer of oxygen-rich alpha-phase titanium on the surface, often referred to as “α-case”.
7. Powder-Based Processes
In terms of powder-based processes, titanium alloys can be produced by both powder metallurgy techniques [157] and, more recently, additive manufacturing techniques [158]. In both cases, the powders can be produced as pre-alloyed [159] or by a blending process [160].
The powder metallurgy processes [159,161,162,163] usually require a shaping process followed by thermal cycles to extract any organic binders (de-binding treatment) and to consolidate the material (sintering). The last treatment is usually carried out at temperatures around 1250 °C, in an inert or vacuum atmosphere. The sintered material usually has good mechanical properties, also due to the controlled microstructure (the microstructure also depends on the powder quality), but often has some residual porosity. In this case, a post-treatment process is required to better consolidate the material using Hot Isostatic Pressing (HIP) [164,165]. The sintered component is usually impregnated at high temperature and pressure using inert gases to mechanically close the residual porosity.
Most of the emerging techniques for producing near-net-shape components using Ti powders are additive manufacturing (3D printing) processes.
The most commonly used techniques are electron beam melting (EBM) [166] and selective laser melting (SLM) [167]. In both cases, the part is created by selectively melting thin layers of powder using a heat source, which can be a laser or an electron beam. In the case of electron beam melting, the process is usually carried out in a vacuum, whereas in the case of SLM, the 3D printing is carried out in a protective atmosphere. The microstructure of 3D-printed parts is strongly influenced by the printing parameters and is completely different for the same material printed by the above-mentioned techniques. While additive manufacturing revolutionizes customization, it may lead to unintended microstructures due to rapid solidification, impacting mechanical properties and biocompatibility [143,144,145]. Stringent control and post-processing, including heat treatments such as hot-isostatic pressing and/or surface modifications, are often necessary in order to mitigate these concerns [146,147]. The as-printed 3D-printed part also has a different surface finish, which is better for the parts produced by SLM. A weak point in terms of mechanical properties is the presence of residual stresses [168,169], which have a strong influence on the fatigue properties of the components, especially for materials produced by the SLM technique. The main advantage of the use of additive manufacturing techniques is the production of components with complex geometries or composed of reticular structures. In particular, the use of reticular structures also makes it possible to control the stiffness of the component to match bone properties [158].
8. Biological Corrosion
One of titanium’s outstanding features is its biocompatibility, which refers to its ability to interact harmoniously with living tissues without eliciting harmful responses. This biocompatibility stems from the oxide layer that spontaneously forms on the surface of titanium upon exposure to air [170]. This oxide layer, primarily composed of titanium dioxide (TiO2), is stable, inert, and effectively isolates the underlying metal from the surrounding biological environment [171]. This phenomenon prevents corrosion and minimizes adverse reactions. In the context of bone and tissue integration, in particular, titanium exhibits excellent osseointegration—direct bonding between bone and implant surface [12]. The oxide layer’s surface chemistry fosters the adsorption of biomolecules like proteins [172], enabling enhanced cell attachment, proliferation, and differentiation. Cells, such as osteoblasts, adhere to the implant surface more readily, promoting bone growth and implant stability. A more in-depth analysis of titanium’s bioactive role will be presented in Section 10.
Alloying elements play a significant role in modulating the susceptibility of titanium alloys to biocorrosion in physiological environments [173,174,175,176]. While most titanium alloys are considered highly resistant to corrosion, certain factors, such as tribocorrosion [177,178] and fretting corrosion [179,180], can introduce complexities. Titanium’s surface, while inherently resistant to corrosion, is susceptible to wear, which can exacerbate corrosion effects in specific conditions.
Alpha-phase titanium alloys, characterized by a high proportion of alpha-phase crystals, are generally more resistant to corrosion due to their stable microstructure [181,182]. In contrast, beta-phase titanium alloys, rich in beta-phase crystals, can be more prone to corrosion, especially in aggressive environments.
Concerns have arisen regarding the potential release of trace elements like vanadium or aluminum from titanium alloys, which could have adverse effects. However, current reports suggest that these releases are minimal, particularly when wear is not a factor. Figure 4 summarizes the relationship between ultimate strength and qualitative corrosion resistance for the most common titanium alloys applied in the biomedical field [43,183].
To enhance the corrosion resistance of titanium alloys, alloying elements such as molybdenum and ruthenium can also be introduced. These elements have demonstrated their ability to improve the alloys’ long-term stability in biological environments. However, the interaction between corrosion resistance, alloy composition, and wear dynamics underscores the intricacies of achieving optimal performance in various medical applications [184,185].
In general, Ti alloys are the biometals less prone to ion release in the human body due to the high stability of the passive films combined with the fastest regeneration of the passive film if destroyed by mechanical damage. No Ti-containing biomolecules have been found in tissues or body fluids in contact with Ti alloy implants [186].
9. Biomedical Applications
Depending on function, size, shape, and anatomical location, different titanium alloys are applied for different types of biomedical devices. The types of biomedical applications will be discussed in this section, and their list can be found in Table 3.
9.1. Dental Implants
The integration of titanium into dental implants and orthodontic braces has revolutionized both fields, significantly improving patient outcomes and comfort [187]. The application of titanium in dentistry finds its roots in the pioneering work of Dr. Per-Ingvar Brånemark, who discovered osseointegration—the direct bond between bone and a titanium surface. This breakthrough not only transformed the landscape of dental implants but also set the stage for the use of titanium in orthodontic applications, such as braces [188].
Titanium dental implants have emerged as the gold standard for replacing missing teeth, in particular as posts [189,190]. The application of titanium posts involves the surgical placement into the jawbone, where, over time, they integrate with the surrounding bone tissue, progressively increasing stability. This integration provides a sturdy foundation for prosthetic teeth, restoring mechanical strength and stability [191], while the upper part of the implant, called the “crown” and made of ceramic or composite materials, restores aesthetics and functionality. Dental implants not only improve chewing and speech but also prevent bone loss, preserving facial structure and overall oral health.
Titanium alloys are also pivotal in orthodontics, where they are used to create braces, wires, and other orthodontic appliances [192,193]. Titanium’s exceptional strength-to-weight ratio and corrosion resistance make it an ideal choice for devices that apply controlled forces to move teeth into proper alignment. Titanium’s biocompatibility ensures that patients tolerate orthodontic treatment well, leading to effective and predictable outcomes.
The oral environment presents a dynamic and challenging milieu for dental implants and orthodontic devices. The oral cavity experiences significant pH fluctuations due to the consumption of various foods and beverages [194]. Acids from acidic foods and drinks can erode tooth enamel and potentially affect the surface of dental devices [19]. Titanium’s corrosion resistance is paramount in combating this challenge, preventing the degradation of the implant surface and ensuring long-term stability.
The oral environment harbors diverse microbial populations, including bacteria. Bacterial colonization on implant surfaces can lead to the formation of biofilms, which pose a threat to device longevity [195,196,197]. While titanium’s biocompatibility discourages bacterial attachment, coatings or modifications may be applied to further deter biofilm formation, ensuring the health of surrounding tissues and the longevity of implants.
Moreover, while mechanical solicitations in the oral environment are generally less severe and geometrically complex compared to orthopedic applications, they are not to be underestimated. Forces from chewing, biting, and speaking subject dental devices to cyclic loading [198,199,200]. Materials must possess sufficient mechanical strength and fatigue resistance to withstand these repetitive stresses over the long term without compromising device integrity.
Long-term clinical studies underscore the success of titanium-based dental devices. Dental implants exhibit impressive survival rates, with 10-year success rates exceeding 95%, according to systematic reviews [201,202,203,204,205,206,207]. Orthodontic appliances made from titanium alloys demonstrate consistent performance, enabling orthodontists to achieve desired tooth movements with a high degree of precision.
Three are the most common alloys applied in the dental field:
β-titanium alloys [192,208,209,210]: These alloys, primarily investigated for dental wires due to their mechanical properties, notably elastic modulus and deformability, encounter limited commercial application;
Ti-6Al-4V [211,212,213,214]: For applications that require very high mechanical strength without compromising biocompatibility, such as in bone plates, screws, fasteners, abutments used for oral implants, and brackets for orthodontic appliances;
9.2. Joint Replacement
From joint replacements to fixation components, titanium’s properties address the complex demands of the musculoskeletal system. This material has enabled the development of implants that seamlessly integrate with bone [13,222], facilitating improved mobility, function, and quality of life for countless individuals. Titanium’s impressive strength, in particular, allows for the creation of robust implants that can withstand physiological loads, ensuring stability and longevity in orthopedic applications [223]. In the history of orthopedic materials, similar results were previously achieved using cobalt–chromium alloys, but titanium presents two critical advantages: it can osseointegrate more easily and it has a higher strength-to-weight ratio, meaning that titanium implants are lighter than cobalt–chromium ones [224,225].
Titanium is used in various joint implants, such as shoulder [226], elbow [227], wrist [228], hip [229], knee [230], and ankle [231]. However, a distinctive aspect of titanium’s use in these implants is that it is never employed as an “articulating component.” This means that titanium is not utilized for the surfaces that directly come into contact and rub against each other within a joint during movement.
The reason for this selective application lies in titanium’s inherent characteristics. While titanium exhibits exceptional biocompatibility, strength, and corrosion resistance, its performance in terms of wear [232] and tribo-corrosion [178] is limited. Titanium’s surfaces are more prone to wear and degradation when subjected to the repetitive, sliding, and abrasive forces present in articulating joint components. This could potentially lead to increased friction, wear debris generation, and even corrosion, which are undesirable outcomes for joint implants aiming to mimic the natural joint’s smooth and efficient movement.
Instead, titanium finds its niche in orthopedics as a material choice for “load-bearing components” within joint implants. For instance, in hip replacements, titanium is often used for the creation of the femoral stem [233] and the acetabular cup [234]. These load-bearing components provide stability and support, transferring the mechanical load from the implant to the surrounding bone. The unique combination of titanium’s flexibility, strength, and light weight is particularly advantageous in these applications, as it enables the implant to withstand physiological loads without compromising the structural integrity of the implant–bone interface.
Apart from joint prostheses, titanium is also used for other, not articulating bone implants, such as ribcages [235] and skull [236] implants, spinal cages, bone scaffolds [237], and support devices. Unlike articulating joint components, which undergo repetitive motion and friction, non-articulating bone implants pose minimal risk of tribological damage. As there are no moving parts or surfaces in contact, the potential for wear, friction-induced debris, or corrosion is significantly reduced. This enhances the longevity and reliability of these fixed devices.
There are various titanium alloys that have been approved for orthopedic uses, but only a limited number of them are utilized in the devices that are actually commercially available. The list is as follows:
Ti-6Al-4V [223,238,239], which is the most widely used titanium alloy in orthopedics, is applied in various load-bearing applications, including hip and knee implants. One of the drawbacks of using Ti-6Al-4V is the potential ion release, as discussed in Section 6, but other concerns include the relatively high elastic modulus, which can be responsible for stress shielding phenomena and consequently bone resorption.
Ti-6Al-7Nb [240,241,242] has a similar biocompatibility and a lower elastic modulus when compared to Ti-6Al-4V, but also a lower mechanical strength. Additionally, its microstructure is more difficult to control.
Ti-15Mo [92,243,244] is used in orthopedics for its corrosion resistance and lower modulus of elasticity. It is employed in applications like spinal implants and bone screws. Its strength is lower compared to Ti-6Al-4V, which may limit its use in high-load scenarios. There are also concerns about the potential release of molybdenum ions in the surrounding biological tissue.
Ti-13Nb-13Zr [245,246,247] is utilized for its biocompatibility and lower Young’s modulus. It is employed in spinal implants, bone plates, and dental applications. It has relatively lower strength compared to other titanium alloys, which can limit its use in high-stress applications.
Commercially pure titanium [248,249,250]: CP Ti is employed for non-load-bearing applications like fixation screws, wires, and plates. Its lower modulus of elasticity reduces stress-shielding effects. Despite the superior biocompatibility, it lacks the high strength of titanium alloys, restricting its use to applications with lower mechanical demands.
Nitinol [251]: the intermetallic compound Nitinol is applied in Mitek suture anchors, which are used to attach soft tissue to the bone.
Overall, titanium alloys used in orthopedic applications have shown very successful clinical outcomes, with some joint implants surviving as long as 30 years or more, despite the challenging environment.
9.3. Trauma Devices
Trauma devices, such as bone plates, screws, and intramedullary nails, require materials that can withstand the mechanical stresses imparted on them within the human body, which can be superior to those faced by orthopedic devices. Moreover, when compared to orthopedic implants, trauma devices are applied in a broader range of anatomical locations and the specific amount of mechanical stress they will encounter can be hard to predict. For this reason, only a limited selection of materials is usually applied in trauma devices, in particular, cobalt–chromium, stainless steel, and titanium, with the latter being the least mechanically performing, in particular, under cyclic fatigue conditions: in a 1996 review of implant failures, the authors noticed that trauma devices made of titanium had five times higher failure rates due to fracture when compared to similar implants made of stainless steel [252] and recommended that the use of titanium devices be limited to less challenging applications. Perren et al., in 2017, noted that titanium plates have generally superior biological properties, have lower chances of adverse reactions, and carry lower risks of infection [253,254]. It must be noted that mechanical irritation through movement of the tissues in relation to the implant surface is also a potential cause for adverse reaction, but it is independent from the material used.
The design of trauma devices [255] with respect to the anatomical location is a key aspect for the success of titanium implants, in particular considering that titanium is a soft metal that can easily produce cytotoxic particulates due to abrasive wear [256].
In screws, including those applied in trauma, the mechanically weakest location is the root of the thread, but thread fractures have never actually been reported in the biomedical literature [257]. Screw shaft fractures, on the other hand, are relatively common. This indicates that the contact forces between bone and thread are relatively weak when compared to the bending solicitations that the shaft faces.
It must be noted that the stress distribution varies greatly in both screws and plates when comparing locking and conventional plates. In locking plates, screws are anchored to the plate itself. Unlike traditional plates where screws rely on friction to hold the bone fragments together, locking plates have special threaded screw holes that completely lock the components together. This locking mechanism provides more stability and minimizes the risk of screw loosening or backing out over time, but it also increases the amount of mechanical stress that both bone and device have to bear [258]. Locking plates are particularly useful in situations where bone quality is poor, as they can provide better fixation in osteoporotic or compromised bone, but they can also cause severe complications such as damage to the surrounding tissues [259].
9.4. Spinal Implants
As previously stated (Section 1), spinal implants are somewhat in the between arthroprosthetic and trauma devices, and their required properties can vary greatly depending on the specific application. Titanium pedicle screws are used to stabilize and immobilize the spine: they are inserted into the vertebral pedicles and serve as anchors for other spinal implant components. Among all the spinal implants, pedicle screws are the ones that have the worst survival rate in vivo [263,264,265], as the diameter of their shaft is limited by the anatomy of the vertebrae, resulting in localized stress intensification.
Titanium rods are often used to connect pedicle screws and provide additional stability to the spine, but due to the higher resisting section, these components are less likely to fail due to mechanical stress. These rods can be contoured to match the curvature of the spine, and this process can lead to fatigue cracking [266], but rod fractures are so uncommon that no systematical follow-up data are available in the literature.
9.5. Cardiovascular Devices
Titanium and its alloys play a crucial role in the development of cardiovascular devices, contributing to improved patient outcomes in the treatment of various heart and vascular conditions. These alloys possess properties that make them well suited for devices aiming to restore normal blood flow, enhance cardiac function, and provide structural support.
Several cardiovascular devices incorporate titanium alloys, including coronary and peripheral vascular stents, devices that are designed to open narrowed or blocked arteries, restoring blood flow and preventing complications like heart attacks, as well as artificial mechanical heart valves, which replace damaged or dysfunctional native tissue and ensure proper blood flow through the heart chambers.
Titanium’s biocompatibility and corrosion resistance make it an excellent choice for enclosures that house pacemakers and implantable cardioverter-defibrillators (ICDs). These enclosures protect sensitive electronics from both the chemically aggressive biological environment and external electromagnetic interferences [273], while minimizing the risk of immune responses [274]. Unlike materials applied for arthroprostetic and trauma devices, the alloys used in pacemakers and defibrillators do not require high mechanical resistance, and the choice of using titanium over other materials is driven purely by chemical resistance and insulation capabilities. Titanium can also be utilized for the electrode tips [275], as an alternative for platinum iridium, titanium nitride, and, more recently, nano-porous carbon [276].
The high mechanical properties of titanium alloys are crucial for other cardiovascular applications, such as in the case of stents and mechanical heart valves.
Cardiovascular stents are medical devices designed to treat various cardiovascular conditions, primarily involving the arteries and blood vessels. These small, tube-like structures are used to help maintain the patency (openness) of narrowed or blocked blood vessels, ensuring a consistent and unobstructed blood flow.
Stents are basically expandable tubes of mesh that are plastically deformed into position. Apart from titanium, good clinical results have been achieved by using AISI 316 Stainless Steel, platinum–iridium alloys, tantalum, and cobalt–chromium alloys [277]. Metals are the main materials utilized for stents because of their mechanical properties and visibility on X-ray imaging [278], but in order to prevent stent restenosis—the re-narrowing or recurrence of blockage in a previously treated blood vessel—the metallic scaffolds are usually coated with hard and anti-adhesive layers such as titanium oxide, titanium nitride [279], and titanium oxynitride [280].
Heart valves present several similitudes with stents, as they are also subjected to mechanical load and require additional coatings to prevent biological interactions. Unlike stents, heart valves are mainly subject to cyclic fatigue and wear [281]. In order to prevent cellular adhesion and proliferation on the valve surface, which might potentially result in an obstruction, heart valves are usually coated with an anti-adherent hard coating such as nanocrystalline diamond [282], diamond-like carbon [283], or titanium oxide [284].
Three titanium alloys have found application in cardiovascular devices:
- -
- -
- -
9.6. Soft Tissue Implants
Titanium is not commonly used as the primary material for soft-tissue implants, which are typically made from materials that are more compatible with the characteristics and flexibility of soft tissues, such as collagen, silk, and various polymers. Soft-tissue implants are designed to mimic the properties of natural soft tissues, such as skin, fat, and muscle, and they are often used for reconstructive or cosmetic surgery.
Despite being more commonly associated with hard-tissue implants, such as those used in orthopedic surgery and dental implants, titanium may, in some cases, be used in combination with other materials or as a component of soft-tissue implants for structural support or anchoring purposes. For instance, titanium meshes may be used to provide support for soft tissues during the healing process or repair [294,295,296]. In soft tissue applications, titanium is commonly utilized as a mesh of wires or, less commonly, as a porous scaffold [297].
Both meshes and scaffolds have superior flexibility when compared to bulk materials, and can display elastic moduli orders of magnitude lower, even if not as low as the soft tissues they are in contact with. As a further drawback, porous structures display lower ultimate strength than their bulk counterparts, which might result in premature failures, in particular, under bending conditions.
10. Biological Functions
The low solubility of titanium in water has been considered the main indicator of its biological inertness. In an oxidizing atmosphere, titanium exists as Ti(IV), and in an aqueous solution is extremely prone to hydrolysis. At the pH of blood (pH 7.4), Ti(IV) compounds dissociate and transform into titanium dioxide, which is considered to be basically insoluble (0.2 fM at pH 7.4) [298,299]. As for other metals, binding by biomolecules in biological fluids actually increases solubility, and several studies suggested values up to about 1 μM in whole blood [300,301]. Some authors have postulated that Ti(IV) can bind to the Fe(III) transport protein sTf, leading to its high organelle bioaccumulation without inhibiting Fe-dependent processes and causing toxicity, while careful delivery can exhibit functions comparable to those of iron [300].
Despite the potential cytotoxicity, since the time of Brånemark, hundreds of thousands of titanium implants have been osseointegrated without complications. This can be explained by taking into consideration that even if soluble, the amount of Ti(IV) released from TiO2 surfaces is virtually negligible, from a biological point of view. It has been suggested that titanium oxide’s capacity for osseointegration is a consequence of the high dielectric constant, which does not cause protein denaturation [302]. Early investigations also supported the hypothesis that the oxide layer incorporates both organic and inorganic material during its growth in vivo [303], providing a transition region between the “pure” implant and the organic material [304]. Molecular dynamics simulations showed that both hydroxylated and nonhydroxylated TiO2 surfaces result in protein–surface electrostatic interactions that are responsible for absorption [305], and the process is faster for hydroxylated surfaces. Experimentally, various proteins such as albumin [306], fibronectin [307], and laminin [308] have been found able to absorb onto titanium dioxide surfaces, proving that adhesion and subsequent osteointegration are indeed regulated by the nanometric passive layer on the outermost surface of titanium implants. Recent publications suggest that the interaction between TiO2 surfaces and proteins is controlled by (I) electrostatic interactions, (II) hydrogen bonding, (III) hydrophobic interactions, and (IV) van der Waals forces:
Divalent cations (mainly calcium) binding can act as a bridge between the negatively charged protein sites (for example R-COO−) and the negatively charged TiO2 surface [309,310];
It was observed that TiO2 bonds with positively charged R-group (lysine, arginine, and histidine) and nonpolar aliphatic R-groups amino acid, but has less affinity for aromatic R-group, polar uncharged R-group, and negatively charged R-group containing amino acids, which suggests that the affinity of TiO2 for amino acids depends on the ability to form stable hydrogen bonds [311,312];
Controlling the hydrophobicity of TiO2 surfaces can increase or reduce protein adhesion and modified hydrophilic TiO2 surfaces displayed anti-fouling capabilities [313];
In most scenarios, Van der Waals forces are complementary to hydrogen bonding, so it is not surprising that both phenomena are usually coupled together [314,315,316].
Apart from cellular adhesion, titanium and, in particular, TiO2 were also reported to be able to stimulate cellular proliferation, probably due to the production of reactive oxygen species (ROS) [315], but, on the other hand, ROS generation induced by TiO2 particles might directly or indirectly damage DNA to cause genotoxicity and impact cellular signaling pathways to modulate cell proliferation, resulting in irreversible cell transformation [317].
Titanium oxide nanoparticles present a high surface area per unit of mass, which in turn increases ROS production and results in a much higher genotoxicity risk [318,319] when compared to bulk titanium implants.
Moreover, as with most biomedical materials, titanium implants elicit an initial inflammatory response as part of the wound-healing process. The interactions include platelet adhesion and mononuclear cell attachment, while mononuclear cells or macrophages interact with the implant and release inflammatory cytokines and chemokines [320]. While an inflammatory response is unavoidable, the levels of cytokine are dependent on many factors, such as anatomical location, surface morphology, chemical composition, and patient conditions [321,322,323].
It has also been observed that the initial adhesion of primary osteoblasts to titanium involves the activation of similar intracellular signaling pathways and gene expression as fibronectin [324] and surface morphology can be further modified to activate phospholipase D1 [325] and other enzymes, meaning that titanium (or better, TiO2) also plays a role in controlling signaling pathways.
11. Long-Term Survival Rates
11.1. Causes of Failure
Titanium implants have a history of long-term success, with devices being able to last up to half a century without the need for revision. Nevertheless, the success of titanium implants strongly depends on how the performances are evaluated and, overall, varies greatly between different applications. For example, the successfulness of a titanium stent depends on the extent of restenosis and the time that occurred between implantation and the next adverse episode, while the successfulness of a spinal device is often evaluated considering how much influence it had on the posture of the patient. Figure 5 resumes the causes for implant failure by splitting them into three categories: mechanical failures such as implant deformation or fracture [326,327], biological failures [328], such as lack of integration or presence of extensive restenosis [329], and infection-related.
All three can occur on all types of biomedical devices, but not with the same probability. Moreover, survival rates greatly depend on the health status of the patient, where age also plays a key role.
11.2. Clinical Follow-Ups
The results of all clinical follow-ups mentioned in this review for patients who were treated with titanium-based biomedical devices are summarized in Figure 6. The type of device has been divided into five categories based on similarity, to simplify interpretation. The results are not divided by cause of revision, which will instead be discussed case by case in the text.
It can be observed that most devices, with the noticeable exception of stents, have a survival rate close to 100% at least in the first few months after implantation. In most cases, early revisions are caused by infections and infections are, overall, relatively uncommon in modern scenarios. Orthopedic implants, for example, reported infection rates below 1% in the first 2 years, in particular for hip articulation [330,331]. Still, risk factors such as obesity, age, presence of diabetes, smoking habits, additional nosocomial infections, wound contamination, preoperative stay, and number of operations were associated with increased risks [332,333,334,335]. The influence of these risk factors has predominantly been explored in the field of orthopedic surgery, where the larger patient cohort provides increased statistical robustness for correlation analyses. Nevertheless, it is reasonable to anticipate that analogous outcomes would likely prevail for various other implant types.
Two additional factors that are often associated with implant infection rates are the geometry of the device (often referred to as “complexity”) [336,337] and the depth of the incision, as implants that are applied closer to the skin seem to incur increased risks of infection [338,339], but statistical correlations have yet to be demonstrated.
For stents, the first few months after implantation appear to be the most critical, as survival rates as low as 87% were reported within the first year [340,341,342,343,344,345]. Most of these early failures appear to be caused by misplacement and migration or in-stent restenosis, but mechanical failures (fractures or inadequate expansions) and infections were also frequently reported.
The region of Figure 6 between a few months and the first 3 years shows more marked differences between the different categories of implants, and the largest statistical dispersions within the same group. Plates and screws, for example, see survival rates as low as 75% and as high as 95% at about 3 years’ follow-up. The statistical dispersion between reported survival rates is mainly associated with patient conditions: specifically designed plates are often used during the reconstruction of bone tissue affected by tumors [346,347], which occasionally results in flap necrosis, plate extrusion, or even fractures [347,348]. Similarly, nails and screws [263,264,265,349,350,351] used in the treatment of metastatic bone fractures can encounter premature failures due to the weakened condition of the surrounding bone tissue [352]. Apart from biological and mechanical failures, the treatment of bone tumors with metallic devices can also result in higher risks of surgical site infections [353].
Low survival rates at about 3 years after implantation were also occasionally reported for stents, and this is again associated with the specific patient cohorts [340,341,342,343,344,345]. Patients requiring a stent often exhibit multiple risk factors that increase the likelihood of implant failure, including conditions such as obesity, diabetes, hypertension, smoking, and a history of cardiovascular diseases [354,355].
In the last region of the graph, going from about 5 to 30 years’ follow-up, most published reports are focused on spinal, dental, and arthroprosthetic implants. These three categories are considered to be the most durable and reliable, but within 10 years, survival rates as low as 70% have been reported for spinal appliances, in particular when associated with vertebral resection due to the presence of tumors [356]. It should also be taken into account that spinal implants have a broad range of scopes, and, consequently, the conditions and probabilities for failure and revision vary greatly. In the treatment of spinal deformities, for example, the outcomes are conventionally assessed by radiographic parameters such as curve size, thoracic and lumbar sagittal plane, and coronal and sagittal balance, which have little to do with the performance of the materials utilized [357]. Artificial discs [358], on the other hand, are probably the best example of spinal devices that have high survival rates at long-term follow-ups. Still, even for reliable implants, the long-term survival rates of spinal implants are in the range of 90% at 10 years [359,360,361].
Despite facing similar potential complications [362,363], dental implants have higher survival rates at longer follow-ups when compared to spinal implants. This is probably caused by the differences in mechanical loading, implant mobility, and also in the conventional failure criteria. Titanium dental implants are often subject to fatigue loading and fretting [364,365], but the stress fields involved are simpler (mostly compression, in the most simple case of titanium posts) and the forces involved are lower [366,367]. Moreover, in the presence of weakened bone tissues, it is relatively easy for the patient to change habits and diet in order to delay the failure of the implant [368,369]. From the chemical and biological point of view, the oral environment is considered to be more aggressive [370,371] than the inside of the body, but also more forgiving.
The longest follow-ups are only available for arthroplasty devices, and most of the reviews published in the literature are actually focused on the hip joint. Results clearly show that titanium arthroprostheses have a high survival rate up to about 10 years of follow-up, but then show a steep decrease between 10 and 30 years. These devices are extremely reliable, and the failure is prevalently caused by patient-associated conditions, such as advanced age [372,373,374,375,376,377,378,379,380,381,382,383,384,385,386,387,388]. Most late failures are caused by osteoporosis and other risk factors that were not present (or not as advanced) at the time of implantation and, overall, mechanical failures and infections only account for about 15% of the total [389].
12. Surface Modification of Titanium
Surface modifications play a crucial role in enhancing the performance and biocompatibility of titanium and its alloys in biomedical applications. In this section, we will provide a list of common strategies for the improvement of the biocompatibility of titanium alloys.
Passivation/Oxidation/anodization: The common aim of these three families of treatments is to control the thickness and chemical composition of the oxide layer that is spontaneously formed on the outermost surface of all titanium alloys. For thin oxide layers, the most important characteristics are chemical stability and uniformity, as their main function is to protect the metal underneath, but when the thickness of the oxide increases to hundreds of nanometers or even microns, the layer can provide additional protection against abrasion and wear, and can be also functionalized with bioactive elements such as calcium and phosphorous [390]. Moreover, as the titanium oxide layer is responsible for protein adhesion and absorption, controlling the thickness and chemical composition can speed up wound healing and implant integration. With the anodizing process, it is also possible to produce nanotubes with controlled dimensions that can increase the surface properties of the implant by enhancing the cell-bone adhesion. In addition, the nanotubes can also be filled with antibacterial medicines to prevent infections.
Hard coatings: Various hard coatings have been applied to titanium alloys, in particular using CVD and PVD, and initially with the intent of increasing the poor tribological resistance [391], in order to be able to use titanium for articulating components such as femoral heads [392,393]. The gap in elastic modulus between the coating and the substrate resulted in early delamination [15] or chipping [394], and consequently an increase in abrasive wear. More reliable results could be achieved by combining together diffusive treatments and PVD coatings [395], but at the expense of fatigue resistance due to the increase in the titanium grain size. In modern applications, hard coatings are mainly applied to reduce cellular adhesion and prevent restenosis in cardiovascular devices [396,397].
Bioactive coatings: Apart from hard coatings, inorganic materials can also be deposited on titanium alloys in order to improve the biological interaction. These coatings can be deposited using a wide array of different techniques, going from plasma spray to electrodeposition, but the most commercial bioactive coatings can basically be referred to in three categories: titanium oxides, calcium compounds, and bioglasses. The properties of TiO2 coatings and their functionalization have been previously discussed in Section 10 and Section 12: Oxidation. For calcium compounds, they represent the most common and successful category of bioactive coatings applied on titanium alloys and include oxides, titanates [398], carbonates [399], phosphates [400], and apatites [401], all of which can be further functionalized by adding small amounts of other atoms or by regulating their crystallinity [402]. Calcium compounds are used in particular for bone integration and regeneration, as they share chemical similarities with the mineral fraction of bone tissues.
Diffusive treatments: Diffusive treatments, such as nitriding and carburizing [395], involve introducing nitrogen or carbon into the surface layer of the titanium alloy through a controlled diffusion process. This creates a hardened surface layer with improved wear resistance, reduced friction, and increased surface hardness. Due to the barrier effect caused both by the native TiO2 layer and the newly formed TiN (or TiC), the diffusion process can take hours or even days before completion [403]. The required time can be reduced by using additional energy sources such as lasers [404], plasmas [405], or ultra-high frequency induction heating [406], but even optimized processes have limitations due to the increased surface roughness [407] and can act as a crack triggering point in fatigue conditions [408].
Physisorption and chemisorption: Growth factors or other biomolecules can be immobilized on the surface of titanium to promote cell attachment, proliferation, and differentiation. This can be achieved through covalent bonding or physical adsorption, and can improve the biological response of the cellular solid in hundreds of different ways [409,410,411]. Such treatments are so different in nature, chemical composition, and application that they will not be discussed in detail in this review.
13. Challenges and Future Directions
While titanium and its alloys have significantly contributed to the advancement of various biomedical fields in the last 60 years, several challenges still persist. First of all, titanium’s relative softness can lead to wear and fretting when in contact with other components (Figure 7). This is not only a major concern for load-bearing implants and articulating surfaces, but also for modular implants where titanium components are connected and interlocked with each other or with harder materials [412,413,414].
Fretting and wear could be reduced by using harder materials, but achieving sufficient hardness while maintaining biocompatibility has been historically challenging. Surface treatments like nitriding [415] and coatings aim to address this issue, but the former requires a long time and often compromises the microstructure, reducing the fatigue resistance and lowering the reliability of the implant in the long term, while the latter often delaminate due to the difference in elastic modulus, also causing third body wear in the process.
Achieving durable and uniform surface modifications that maintain their properties over time remains a challenge and even if new solutions are constantly proposed in the scientific literature, they seem to never reach the necessary maturity to be transferred to industrial applications.
While titanium’s inertness reduces infection risks, biofilm formation also remains a concern [196], in particular for modern, cellular solid materials and scaffolds that present a high area per unit of volume [416]. These devices can be hard to sterilize using “directional” sources like UV or gamma rays [417].
Despite being more complex to sterilize, cellular solids and scaffolds can mimic the structure and properties of natural tissues to encourage seamless integration and minimize foreign body response. This is in particular possible thanks to the various additive manufacturing technologies nowadays available on the market [418]. The constant improvement of such techniques will also create new potential applications for titanium alloys, in particular for custom-made devices, while the increase in achievable resolution will open new market opportunities for smaller implantable devices and sensors.
14. Advantages and Disadvantages
As we have seen in the previous sections, titanium and its alloys have become indispensable materials in biomedical applications, contributing significantly to the success of various medical devices and implants. In particular, independent of their application, titanium alloys exhibit excellent biocompatibility [419], minimizing the risk of adverse reactions when in contact with biological tissues, even under challenging biological loads and often decades after they were implanted. Moreover, unlike other successful structural biomaterials such as alumina, titanium alloys are not simply bio-inert, as they have been proven to be able to osseointegrate [420], providing additional support and stability to the implant over time.
Despite the extremely positive outcomes and the encouraging results of decades-long follow-ups, the use of titanium alloys in the biomedical field does have a few major disadvantages: titanium is expensive to produce [421] (about 15 times more expensive than medical-grade AISI 316L stainless steel), difficult to machine, easily damaged by wear, and also much heavier and stiffer than bone. Moreover, concerns are still raised about its biological stability, either because of the potential release of harmful ions over time or because of the low but not negligible risk of allergic reactions [422].
Over the years, innovative alloys with lower elastic modules [423], but not containing harmful elements, were developed. Ti-13Nb-13Zr [245,246,247], for example, has comparable mechanical properties but superior biocompatibility and a lower elastic modulus when compared to the most common Ti-6Al-4V alloy. Extensive research and experience have accumulated over decades with Ti-6Al-4V, leading to well-established manufacturing processes, quality control procedures, and design guidelines. In contrast, alloys like Ti-13Nb-13Zr are still relatively new, with ongoing research and development [424].
Other biocompatible metallic alloys, such as cobalt chromium and stainless steel, have superior wear resistance and mechanical properties, but also higher elastic moduli and, overall, generate more concerns about their biocompatibility [425]. In considering alternative materials for various biomedical applications, high-performance polymers are a viable option [426]. These polymers offer a compelling combination of good biocompatibility and mechanical properties that can closely mimic those of natural bone [427,428,429]. Moreover, the ease with which they can be functionalized enhances their versatility in biomedical engineering [430,431]. While high-performance polymers present promising alternatives for many practical applications, there are instances where the mechanical robustness of titanium makes it the more reliable choice, such as femoral stems or nails.
15. Conclusions
The evolution of titanium and its alloys in the biomedical field has transformed the landscape of medical engineering and patient care. From the pioneering work of Dr. Per-Ingvar Brånemark to the present day, titanium’s exceptional properties have catalyzed innovations in orthopedics, dental care, cardiovascular interventions, soft tissue implants, and beyond. The exceptional combination of the biocompatibility, corrosion resistance, and mechanical strength of titanium has enabled the development of implants that seamlessly integrate with the body, promoting healing, mobility, and a better quality of life for patients.
However, as this review has highlighted, challenges persist. The field is actively addressing concerns such as wear, surface modifications, infection prevention, and the need for improved integration with soft tissues. The quest for innovation remains fueled by a pursuit of durability, precision, personalization, and enhanced functionalities.
As researchers, clinicians, and engineers bridge disciplines, synergies emerge, bringing forth solutions that redefine the boundaries of medical possibilities. Titanium’s legacy in the biomedical field stands as a testament to human ingenuity, the pursuit of excellence, and the unwavering commitment to advancing healthcare for the betterment of humanity. As this remarkable journey unfolds, titanium remains a steadfast ally, propelling medical science toward new horizons.
Author Contributions
Conceptualization, E.M. and A.L.; methodology, E.M. and A.L.; validation, E.M. and A.L.; formal analysis, E.M. and A.L.; resources, E.M. and A.L.; data curation, E.M. and A.L.; writing—original draft preparation, E.M. and A.L.; writing—review and editing, E.M. and A.L.; visualization, E.M. and A.L.; project administration, E.M. and A.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing is not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Blackwood, D.J. Biomaterials: Past Successes and Future Problems. Corros. Rev. 2003, 21, 97–124. [Google Scholar] [CrossRef]
- Elias, C.N.; Fernandes, D.J.; de Souza, F.M.; Monteiro, E.D.S.; de Biasi, R.S. Mechanical and Clinical Properties of Titanium and Titanium-Based Alloys (Ti G2, Ti G4 Cold Worked Nanostructured and Ti G5) for Biomedical Applications. J. Mater. Res. Technol. 2019, 8, 1060–1069. [Google Scholar] [CrossRef]
- Kaur, M.; Singh, K. Review on Titanium and Titanium Based Alloys as Biomaterials for Orthopaedic Applications. Mater. Sci. Eng. C Mater. Biol. Appl. 2019, 102, 844–862. [Google Scholar] [CrossRef] [PubMed]
- Tomashov, N.D.; Altovsky, R.M.; Chernova, G.P. Passivity and Corrosion Resistance of Titanium and Its Alloys. J. Electrochem. Soc. 1961, 108, 113. [Google Scholar] [CrossRef]
- Bosshardt, D.D.; Chappuis, V.; Buser, D. Osseointegration of Titanium, Titanium Alloy and Zirconia Dental Implants: Current Knowledge and Open Questions. Periodontol. 2000 2017, 73, 22–40. [Google Scholar] [CrossRef]
- Zhang, L.-C.; Chen, L.-Y. A Review on Biomedical Titanium Alloys: Recent Progress and Prospect. Adv. Eng. Mater. 2019, 21, 1801215. [Google Scholar] [CrossRef]
- Quinn, J.; McFadden, R.; Chan, C.-W.; Carson, L. Titanium for Orthopedic Applications: An Overview of Surface Modification to Improve Biocompatibility and Prevent Bacterial Biofilm Formation. iScience 2020, 23, 101745. [Google Scholar] [CrossRef]
- Jorge, J.R.P.; Barão, V.A.; Delben, J.A.; Faverani, L.P.; Queiroz, T.P.; Assunção, W.G. Titanium in Dentistry: Historical Development, State of the Art and Future Perspectives. J. Indian Prosthodont. Soc. 2013, 13, 71–77. [Google Scholar] [CrossRef]
- Olin, C. Titanium in Cardiac and Cardiovascular Applications. In Engineering Materials; Springer: Berlin/Heidelberg, Germany, 2001; pp. 889–907. ISBN 9783642631191. [Google Scholar]
- Mishra, S.K.; Chowdhary, R.; Chrcanovic, B.R.; Brånemark, P.-I. Osseoperception in Dental Implants: A Systematic Review. J. Prosthodont. 2016, 25, 185–195. [Google Scholar] [CrossRef]
- Tjellström, A.; Lindström, J.; Hallén, O.; Albrektsson, T.; Brånemark, P.I. Osseointegrated Titanium Implants in the Temporal Bone. A Clinical Study on Bone-Anchored Hearing Aids. Am. J. Otol. 1981, 2, 304–310. [Google Scholar]
- Carlsson, L.; Röstlund, T.; Albrektsson, B.; Albrektsson, T.; Brånemark, P.I. Osseointegration of Titanium Implants. Acta Orthop. Scand. 1986, 57, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Zaid, M.B.; O’Donnell, R.J.; Potter, B.K.; Forsberg, J.A. Orthopaedic Osseointegration: State of the Art. J. Am. Acad. Orthop. Surg. 2019, 27, e977–e985. [Google Scholar] [CrossRef] [PubMed]
- Marin, E.; Fedrizzi, L.; Zagra, L. Porous Metallic Structures for Orthopaedic Applications: A Short Review of Materials and Technologies. Eur. Orthop. Traumatol. 2010, 1, 103–109. [Google Scholar] [CrossRef]
- Raimondi, M.T.; Pietrabissa, R. The In-Vivo Wear Performance of Prosthetic Femoral Heads with Titanium Nitride Coating. Biomaterials 2000, 21, 907–913. [Google Scholar] [CrossRef]
- Lalor, P.A.; Revell, P.A.; Gray, A.B.; Wright, S.; Railton, G.T.; Freeman, M.A. Sensitivity to Titanium. A Cause of Implant Failure? J. Bone Jt. Surg. Br. 1991, 73, 25–28. [Google Scholar] [CrossRef]
- Jacobs, J.J.; Silverton, C.; Hallab, N.J.; Skipor, A.K.; Patterson, L.; Black, J.; Galante, J.O. Metal Release and Excretion from Cementless Titanium Alloy Total Knee Replacements. Clin. Orthop. Relat. Res. 1999, 358, 173–180. [Google Scholar] [CrossRef]
- Onisi, M.; Kondo, W. Establishing an Environment for Growth of Aciduric Bacteria in the Oral Cavity. J. Dent. Res. 1956, 35, 596–602. [Google Scholar] [CrossRef]
- Pezzotti, G.; Adachi, T.; Gasparutti, I.; Vincini, G.; Zhu, W.; Boffelli, M.; Rondinella, A.; Marin, E.; Ichioka, H.; Yamamoto, T.; et al. Vibrational Monitor of Early Demineralization in Tooth Enamel after in Vitro Exposure to Phosphoridic Liquid. Spectrochim. Acta A Mol. Biomol. Spectrosc. 2017, 173, 19–33. [Google Scholar] [CrossRef]
- White, D.J. Dental Calculus: Recent Insights into Occurrence, Formation, Prevention, Removal and Oral Health Effects of Supragingival and Subgingival Deposits. Eur. J. Oral Sci. 1997, 105, 508–522. [Google Scholar] [CrossRef]
- Takahashi, N. Microbial Ecosystem in the Oral Cavity: Metabolic Diversity in an Ecological Niche and Its Relationship with Oral Diseases. Int. Congr. Ser. 2005, 1284, 103–112. [Google Scholar] [CrossRef]
- Leban, M.B.; Kosec, T.; Finšgar, M. Corrosion Characterization and Ion Release in SLM-Manufactured and Wrought Ti6Al4V Alloy in an Oral Environment. Corros. Sci. 2022, 209, 110716. [Google Scholar] [CrossRef]
- Ramazanzadeh, B.A.; Ahrari, F.; Sabzevari, B.; Habibi, S. Nickel Ion Release from Three Types of Nickel-Titanium-Based Orthodontic Archwires in the as-Received State and after Oral Simulation. J. Dent. Res. Dent. Clin. Dent. Prospects 2014, 8, 71–76. [Google Scholar] [PubMed]
- Barber, C.C.; Burnham, M.; Ojameruaye, O.; McKee, M.D. A Systematic Review of the Use of Titanium versus Stainless Steel Implants for Fracture Fixation. OTA Int. 2021, 4, e138. [Google Scholar] [CrossRef] [PubMed]
- Gugala, Z.; Lindsey, R.W. Removal versus Retention of Orthopaedic Trauma Implants. Orthop. Knowl. Online 2015, 13, 1–20. [Google Scholar] [CrossRef]
- Vos, D.; Hanson, B.; Verhofstad, M. Implant Removal of Osteosynthesis: The Dutch Practice. Results of a Survey. J. Trauma Manag. Outcomes 2012, 6, 6. [Google Scholar] [CrossRef]
- Hayes, J.S.; Seidenglanz, U.; Pearce, A.I.; Pearce, S.G.; Archer, C.W.; Richards, R.G. Surface Polishing Positively Influences Ease of Plate and Screw Removal. Eur. Cell. Mater. 2010, 19, 117–126. [Google Scholar] [CrossRef]
- Carlsson, L.; Röstlund, T.; Albrektsson, B.; Albrektsson, T. Removal Torques for Polished and Rough Titanium Implants. Int. J. Oral Maxillofac. Implants 1988, 3, 21–24. [Google Scholar]
- Elias, W.J.; Simmons, N.E.; Kaptain, G.J.; Chadduck, J.B.; Whitehill, R. Complications of Posterior Lumbar Interbody Fusion When Using a Titanium Threaded Cage Device. J. Neurosurg. 2000, 93, 45–52. [Google Scholar] [CrossRef]
- Boelderl, A.; Daniaux, H.; Kathrein, A.; Maurer, H. Danger of Damaging the Medial Branches of the Posterior Rami of Spinal Nerves during a Dorsomedian Approach to the Spine. Clin. Anat. 2002, 15, 77–81. [Google Scholar] [CrossRef]
- Warburton, A.; Girdler, S.J.; Mikhail, C.M.; Ahn, A.; Cho, S.K. Biomaterials in Spinal Implants: A Review. Neurospine 2020, 17, 101–110. [Google Scholar] [CrossRef]
- Smit, T.H.; Müller, R.; van Dijk, M.; Wuisman, P.I.J.M. Changes in Bone Architecture during Spinal Fusion: Three Years Follow-up and the Role of Cage Stiffness. Spine (Phila. Pa. 1976) 2003, 28, 1802–1808; Discussion 1809. [Google Scholar] [CrossRef] [PubMed]
- Myerburg, R.J.; Feigal, D.W., Jr.; Lindsay, B.D. Life-Threatening Malfunction of Implantable Cardiac Devices. N. Engl. J. Med. 2006, 354, 2309–2311. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, J.C. Crystal Structures of Titanium, Zirconium, and Hafnium at High Pressures. Science 1963, 140, 72–73. [Google Scholar] [CrossRef] [PubMed]
- Del Castillo, R.; Chochlidakis, K.; Galindo-Moreno, P.; Ercoli, C. Titanium Nitride Coated Implant Abutments: From Technical Aspects and Soft Tissue Biocompatibility to Clinical Applications. A Literature Review. J. Prosthodont. 2022, 31, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Mertens, T.; Kollek, H. On the Stability and Composition of Oxide Layers on Pre-Treated Titanium. Int. J. Adhes. Adhes. 2010, 30, 466–477. [Google Scholar] [CrossRef]
- Cunha, A.; Renz, R.P.; Blando, E.; de Oliveira, R.B.; Hübler, R. Osseointegration of Atmospheric Plasma-Sprayed Titanium Implants: Influence of the Native Oxide Layer. J. Biomed. Mater. Res. A 2014, 102, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Akai, A.; Shiozawa, D.; Sakagami, T. Fatigue Limit Estimation of Titanium Alloy Ti-6Al-4V with Infrared Thermography. In Proceedings of the Thermosense: Thermal Infrared Applications XXXIX, Anaheim, CA, USA, 5 May 2017; Bison, P., Burleigh, D., Eds.; SPIE: Bellingham, WA, USA, 2017. [Google Scholar]
- Teoh, S. Fatigue of Biomaterials: A Review. Int. J. Fatigue 2000, 22, 825–837. [Google Scholar] [CrossRef]
- Kopp, C.D. Brånemark Osseointegration. Prognosis and Treatment Rationale. Dent. Clin. N. Am. 1989, 33, 701–731. [Google Scholar] [CrossRef]
- Brånemark, R.; Brånemark, P.I.; Rydevik, B.; Myers, R.R. Osseointegration in Skeletal Reconstruction and Rehabilitation: A Review. J. Rehabil. Res. Dev. 2001, 38, 175–181. [Google Scholar]
- Odman, J.; Lekholm, U.; Jemt, T.; Brånemark, P.I.; Thilander, B. Osseointegrated Titanium Implants—A New Approach in Orthodontic Treatment. Eur. J. Orthod. 1988, 10, 98–105. [Google Scholar] [CrossRef]
- Martín-Cameán, A.; Jos, A.; Puerto, M.; Calleja, A.; Iglesias-Linares, A.; Solano, E.; Cameán, A.M. In Vivo Determination of Aluminum, Cobalt, Chromium, Copper, Nickel, Titanium and Vanadium in Oral Mucosa Cells from Orthodontic Patients with Mini-Implants by Inductively Coupled Plasma-Mass Spectrometry (ICP-MS). J. Trace Elem. Med. Biol. 2015, 32, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Shabalovskaya, S.; Anderegg, J.; Van Humbeeck, J. Critical Overview of Nitinol Surfaces and Their Modifications for Medical Applications. Acta Biomater. 2008, 4, 447–467. [Google Scholar] [CrossRef] [PubMed]
- Sohn, H.-S. Production Technology of Titanium by Kroll Process. J. Korean Inst. Resour. Recycl. 2020, 29, 3–14. [Google Scholar] [CrossRef]
- Agripa, H.; Botef, I. Modern Production Methods for Titanium Alloys: A Review. In Titanium Alloys—Novel Aspects of Their Manufacturing and Processing; IntechOpen: London, UK, 2019. [Google Scholar]
- Woodside, C.R.; King, P.E.; Nordlund, C. Arc Distribution during the Vacuum Arc Remelting of Ti-6Al-4V. Metall. Mater. Trans. B 2013, 44, 154–165. [Google Scholar] [CrossRef]
- Blackburn, M.J.; Malley, D.R. Plasma Arc Melting of Titanium Alloys. Mater. Eng. 1993, 14, 19–27. [Google Scholar] [CrossRef]
- Fashu, S.; Lototskyy, M.; Davids, M.W.; Pickering, L.; Linkov, V.; Tai, S.; Renheng, T.; Fangming, X.; Fursikov, P.V.; Tarasov, B.P. A Review on Crucibles for Induction Melting of Titanium Alloys. Mater. Des. 2020, 186, 108295. [Google Scholar] [CrossRef]
- Fang, Z.Z.; Paramore, J.D.; Sun, P.; Chandran, K.S.R.; Zhang, Y.; Xia, Y.; Cao, F.; Koopman, M.; Free, M. Powder Metallurgy of Titanium—Past, Present, and Future. Int. Mater. Rev. 2018, 63, 407–459. [Google Scholar] [CrossRef]
- Chan, K.S.; Koike, M.; Johnson, B.W.; Okabe, T. Modeling of Alpha-Case Formation and Its Effects on the Mechanical Properties of Titanium Alloy Castings. Metall. Mater. Trans. A 2008, 39, 171–180. [Google Scholar] [CrossRef]
- Gaddam, R.; Sefer, B.; Pederson, R.; Antti, M.-L. Study of Alpha-Case Depth in Ti-6Al-2Sn-4Zr-2Mo and Ti-6Al-4V. IOP Conf. Ser. Mater. Sci. Eng. 2013, 48, 012002. [Google Scholar] [CrossRef]
- Eisenbarth, E.; Velten, D.; Müller, M.; Thull, R.; Breme, J. Biocompatibility of Beta-Stabilizing Elements of Titanium Alloys. Biomaterials 2004, 25, 5705–5713. [Google Scholar] [CrossRef]
- Li, Y.; Wong, C.; Xiong, J.; Hodgson, P.; Wen, C. Cytotoxicity of Titanium and Titanium Alloying Elements. J. Dent. Res. 2010, 89, 493–497. [Google Scholar] [CrossRef]
- Abdel-Hady Gepreel, M.; Niinomi, M. Biocompatibility of Ti-Alloys for Long-Term Implantation. J. Mech. Behav. Biomed. Mater. 2013, 20, 407–415. [Google Scholar] [CrossRef]
- Bania, P.J. Beta Titanium Alloys and Their Role in the Titanium Industry. JOM 1994, 46, 16–19. [Google Scholar] [CrossRef]
- Gupta, R.K.; Pant, B.; Sinha, P.P. Theory and Practice of γ + A2 Ti Aluminide: A Review. Trans. Indian Inst. Met. 2014, 67, 143–165. [Google Scholar] [CrossRef]
- Kim, Y.-W. Gamma Titanium Aluminides. JOM 1995, 47, 38. [Google Scholar] [CrossRef]
- Duwez, P. The Martensite Transformation Temperature in Titanium Binary Alloys. Trans. ASME J. Appl. Mech. 1953, 45, 934–940. [Google Scholar]
- Ivasishin, O.M.; Teliovich, R.V. Transformation Plasticity in Titanium Alpha Double Prime Martensite. J. Phys. IV 2001, 11, Pr4-165–Pr4-172. [Google Scholar] [CrossRef]
- Hickman, B.S. The Formation of Omega Phase in Titanium and Zirconium Alloys: A Review. J. Mater. Sci. 1969, 4, 554–563. [Google Scholar] [CrossRef]
- Weiss, I.; Semiatin, S.L. Thermomechanical Processing of Alpha Titanium Alloys—An Overview. Mater. Sci. Eng. A Struct. Mater. 1999, 263, 243–256. [Google Scholar] [CrossRef]
- Koul, M.K.; Breedis, J.F. Phase Transformations in Beta Isomorphous Titanium Alloys. Acta Metall. 1970, 18, 579–588. [Google Scholar] [CrossRef]
- Mwinteribo, T.V.; Li, C.; Saifu, W.; Li, J.; Xu, X. Mechanical Properties of near Alpha Titanium Alloys for High-Temperature Applications—A Review. Aircr. Eng. Aerosp. Technol. 2020, 92, 521–540. [Google Scholar]
- Semiatin, S.L.; Seetharaman, V.; Weiss, I. The Thermomechanical Processing of Alpha/Beta Titanium Alloys. JOM 1997, 49, 33–39. [Google Scholar] [CrossRef]
- Liu, Y.; Lim, S.C.V.; Ding, C.; Huang, A.; Weyland, M. Unravelling the Competitive Effect of Microstructural Features on the Fracture Toughness and Tensile Properties of near Beta Titanium Alloys. J. Mater. Sci. Technol. 2022, 97, 101–112. [Google Scholar] [CrossRef]
- Sidhu, S.S.; Singh, H.; Gepreel, M.A.-H. A Review on Alloy Design, Biological Response, and Strengthening of β-Titanium Alloys as Biomaterials. Mater. Sci. Eng. C Mater. Biol. Appl. 2021, 121, 111661. [Google Scholar] [CrossRef]
- Alipour, S.; Taromian, F.; Ghomi, E.R.; Zare, M.; Singh, S.; Ramakrishna, S. Nitinol: From Historical Milestones to Functional Properties and Biomedical Applications. Proc. Inst. Mech. Eng. H 2022, 236, 1595–1612. [Google Scholar] [CrossRef]
- Elias, C.N.; Lima, J.H.C.; Valiev, R.; Meyers, M.A. Biomedical Applications of Titanium and Its Alloys. JOM 2008, 60, 46–49. [Google Scholar] [CrossRef]
- Elias, C.N.; Meyers, M.A.; Valiev, R.Z.; Monteiro, S.N. Ultrafine Grained Titanium for Biomedical Applications: An Overview of Performance. J. Mater. Res. Technol. 2013, 2, 340–350. [Google Scholar] [CrossRef]
- Marin, E.; Pressacco, M.; Fusi, S.; Lanzutti, A.; Turchet, S.; Fedrizzi, L. Characterization of Grade 2 Commercially Pure Trabecular Titanium Structures. Mater. Sci. Eng. C Mater. Biol. Appl. 2013, 33, 2648–2656. [Google Scholar] [CrossRef]
- Ohkubo, C.; Shimura, I.; Aoki, T.; Hanatani, S.; Hosoi, T.; Okabe, T. In Vitro Wear Assessment of Titanium Alloy Teeth. J. Prosthodont. 2002, 11, 263–269. [Google Scholar] [CrossRef]
- Atapour, M.; Pilchak, A.L.; Shamanian, M.; Fathi, M.H. Corrosion Behavior of Ti–8Al–1Mo–1V Alloy Compared to Ti–6Al–4V. Mater. Eng. 2011, 32, 1692–1696. [Google Scholar] [CrossRef]
- Sabarish, S.; Kumar, P.U. Prototyping and Analysis of Knee Implant by Rapid Prototyping. Available online: https://www.academia.edu/ (accessed on 15 October 2023).
- Che Lah, N.A.; Hussin, M.H. Titanium and Titanium Based Alloys as Metallic Biomaterials in Medical Applications-Spine Implant Case Study. Pertanika J. Sci. Technol. 2019, 27, 459–472. [Google Scholar]
- Izri, Z.; Bijanzad, A.; Torabnia, S.; Lazoglu, I. In Silico Evaluation of Lattice Designs for Additively Manufactured Total Hip Implants. Comput. Biol. Med. 2022, 144, 105353. [Google Scholar] [CrossRef]
- Mohseni, E.; Zalnezhad, E.; Bushroa, A.R. Comparative Investigation on the Adhesion of Hydroxyapatite Coating on Ti–6Al–4V Implant: A Review Paper. Int. J. Adhes. Adhes. 2014, 48, 238–257. [Google Scholar] [CrossRef]
- Niu, W.; Bermingham, M.J.; Baburamani, P.S.; Palanisamy, S.; Dargusch, M.S.; Turk, S.; Grigson, B.; Sharp, P.K. The Effect of Cutting Speed and Heat Treatment on the Fatigue Life of Grade 5 and Grade 23 Ti–6Al–4V Alloys. Mater. Eng. 2013, 46, 640–644. [Google Scholar] [CrossRef]
- Sun, Y.; Huang, B.; Puleo, D.A.; Schoop, J.; Jawahir, I.S. Improved Surface Integrity from Cryogenic Machining of Ti-6Al-7Nb Alloy for Biomedical Applications. Procedia CIRP 2016, 45, 63–66. [Google Scholar] [CrossRef]
- Assis, S.L.; Costa, I. Electrochemical Evaluation of Ti-13Nb-13Zr, Ti-6Al-4V and Ti-6Al-7Nb Alloys for Biomedical Application by Long-Term Immersion Tests. Mater. Corros. 2007, 58, 329–333. [Google Scholar] [CrossRef]
- Chandler, H. Heat Treater’s Guide: Practices and Procedures for Nonferrous Alloys; ASM International: Almere, The Netherlands, 1996; ISBN 9780871705655. [Google Scholar]
- Canelo-Yubero, D.; Poletti, C.; Warchomicka, F.; Daniels, J.; Requena, G. Load Partition and Microstructural Evolution during Hot Deformation of Ti-6Al-6V-2Sn Matrix Composites, and Possible Strengthening Mechanisms. J. Alloy. Compd. 2018, 764, 937–946. [Google Scholar] [CrossRef]
- Carrozza, A.; Aversa, A.; Fino, P.; Lombardi, M. Towards Customized Heat Treatments and Mechanical Properties in the LPBF-Processed Ti-6Al-2Sn-4Zr-6Mo Alloy. Mater. Des. 2022, 215, 110512. [Google Scholar] [CrossRef]
- Li, H.-M.; Li, M.-Q.; Luo, J.; Wang, K. Microstructure and Mechanical Properties of Heat-Treated Ti–5Al–2Sn–2Zr–4Mo–4Cr. Trans. Nonferrous Met. Soc. China 2015, 25, 2893–2900. [Google Scholar] [CrossRef]
- Kharia, K.K.; Rack, H.J. Martensitic Phase Transformations in IMI 550 (Ti-4Al-4Mo-2Sn-0.5 Si). Metall. Mater. Trans. A 2001, 32, 671–679. [Google Scholar] [CrossRef]
- Yu, S.; Yu, Z.-T.; Han, J.-Y.; Wang, G.; Niu, J.-L.; Dargusch, M.S. Haemocompatibility of Ti–3Zr–2Sn–3Mo–25Nb Biomedical Alloy with Surface Heparinization Using Electrostatic Self Assembly Technology. Trans. Nonferrous Met. Soc. China 2012, 22, 3046–3052. [Google Scholar] [CrossRef]
- Yang, X.; Hutchinson, C.R. Corrosion-Wear of β-Ti Alloy TMZF (Ti-12Mo-6Zr-2Fe) in Simulated Body Fluid. Acta Biomater. 2016, 42, 429–439. [Google Scholar] [CrossRef]
- Yang, X. Mechanical Behaviour of Ti-12Mo-6Zr-2Fe (TMZF) β-Titanium Alloy in Physiological Environments. Doctoral Dissertation, Monash University, Melbourne, Australia, 2017. [Google Scholar]
- Wang, K. The Characterization of Ti-12Mo-6Zr-2Fe A New Biocompatible Titanium Alloy Developed for Surgical Implant. Beta Titanium Alloys in the 1990’s. In Proceedings of the 122 Annual Meeting of the Minerals, Metals and Materials Society (TMS), Denver, CO, USA, 21–25 February 1993; pp. 46–60, ISBN 0-87339-200-0. [Google Scholar]
- Fellah, M.; Hezil, N.; Leila, D.; Abdul Samad, M.; Djellabi, R.; Kosman, S.; Montagne, A.; Iost, A.; Obrosov, A.; Weiss, S. Effect of Sintering Temperature on Structure and Tribological Properties of Nanostructured Ti–15Mo Alloy for Biomedical Applications. Trans. Nonferrous Met. Soc. China 2019, 29, 2310–2320. [Google Scholar] [CrossRef]
- Kumar, S.; Narayanan, T.S.N.S. Corrosion Behaviour of Ti-15Mo Alloy for Dental Implant Applications. J. Dent. 2008, 36, 500–507. [Google Scholar] [CrossRef]
- Zardiackas, L.D.; Mitchell, D.W.; Disegi, J.A. Characterization of Ti-15Mo Beta Titanium Alloy for Orthopaedic Implant Applications. In Medical Applications of Titanium and Its Alloys: The Material and Biological Issues; ASTM International: West Conshohocken, PA, USA, 2009; pp. 60–75. ISBN 9780803120105. [Google Scholar]
- Sun, S.H.; Hagihara, K.; Ishimoto, T.; Suganuma, R.; Xue, Y.F.; Nakano, T. Comparison of Microstructure, Crystallographic Texture, and Mechanical Properties in Ti-15Mo-5Zr-3Al Alloys Fabricated via Electron and Laser Beam Powder Bed Fusion Technologies. Addit. Manuf. 2021, 47, 102329. [Google Scholar] [CrossRef]
- Ishimoto, T.; Hagihara, K.; Hisamoto, K.; Sun, S.-H.; Nakano, T. Crystallographic Texture Control of Beta-Type Ti–15Mo–5Zr–3Al Alloy by Selective Laser Melting for the Development of Novel Implants with a Biocompatible Low Young’s Modulus. Scr. Mater. 2017, 132, 34–38. [Google Scholar] [CrossRef]
- Bhambri, S.K.; Shetty, R.H.; Gilbertson, L.N. Optimization of Properties of Ti-15Mo-2.8 Nb-3Al-0.2 Si & Ti-15Mo-2.8 Nb-0.2 Si-. 260 Beta Titanium Alloys for Application in Prosthetic Implants. Astm Spec. Tech. Publ. 1996, 1272, 88–95. [Google Scholar]
- Niinomi, M.; Hattori, T.; Niwa, S. Material Characteristics and Biocompatibility of Low Rigidity Titanium Alloys for Biomedical Applications. In Biomaterials in Orthopedics; Informa Healthcare: London, UK, 2003; ISBN 9780824742942. [Google Scholar]
- Zhou, Y.L.; Niinomi, M.; Akahori, T. Dynamic Young’s Modulus and Mechanical Properties of Ti−Hf Alloys. Mater. Trans. 2004, 45, 1549–1554. [Google Scholar] [CrossRef]
- Zhou, Y.-L.; Niinomi, M. Passive Films and Corrosion Resistance of Ti–Hf Alloys in 5% HCl Solution. Surf. Coat. Technol. 2009, 204, 180–186. [Google Scholar] [CrossRef]
- Bhola, R.; Bhola, S.M.; Mishra, B.; Ayers, R.A.; Olson, D.L.; Thompson, D.O.; Chimenti, D.E. Electrochemical Characterization of A Low Modulus Ti-35.5nb-7.3zr-5.7ta Alloy in A Simulated Body Fluid Using EIS for Biomedical Applications; AIP: College Park, ML, USA, 2011. [Google Scholar]
- Correa, D.R.N.; Rocha, L.A.; Donato, T.A.G.; Sousa, K.S.J.; Grandini, C.R.; Afonso, C.R.M.; Doi, H.; Tsutsumi, Y.; Hanawa, T. On the Mechanical Biocompatibility of Ti-15Zr-Based Alloys for Potential Use as Load-Bearing Implants. J. Mater. Res. Technol. 2020, 9, 1241–1250. [Google Scholar] [CrossRef]
- Niinomi, M. Fatigue Performance and Cyto-Toxicity of Low Rigidity Titanium Alloy, Ti-29Nb-13Ta-4.6Zr. Biomaterials 2003, 24, 2673–2683. [Google Scholar] [CrossRef]
- Hao, Y.L.; Yang, R.; Niinomi, M.; Kuroda, D.; Zhou, Y.L.; Fukunaga, K.; Suzuki, A. Aging Response of the Young’s Modulus and Mechanical Properties of Ti-29Nb-13Ta-4.6 Zr for Biomedical Applications. Metall. Mater. Trans. A 2003, 34, 1007–1012. [Google Scholar] [CrossRef]
- Ikeda, M.; Komatsu, S.-Y.; Sowa, I.; Niinomi, M. Aging Behavior of the Ti-29Nb-13Ta-4.6Zr New Beta Alloy for Medical Implants. Metall. Mater. Trans. A 2002, 33, 487–493. [Google Scholar] [CrossRef]
- Li, X.; Ye, S.; Yuan, X.; Yu, P. Fabrication of Biomedical Ti-24Nb-4Zr-8Sn Alloy with High Strength and Low Elastic Modulus by Powder Metallurgy. J. Alloys Compd. 2019, 772, 968–977. [Google Scholar] [CrossRef]
- Santos, P.F.; Niinomi, M.; Liu, H.; Cho, K.; Nakai, M.; Itoh, Y.; Narushima, T.; Ikeda, M. Fabrication of Low-Cost Beta-Type Ti-Mn Alloys for Biomedical Applications by Metal Injection Molding Process and Their Mechanical Properties. J. Mech. Behav. Biomed. Mater. 2016, 59, 497–507. [Google Scholar] [CrossRef]
- Santos, P.; Niinomi, M.; Cho, K.; Nakai, M.; Liu, H. Development of New Ti-Mn-Mo Alloys for Use in Biomedical Applications. In Proceedings of the 13th World Conference on Titanium; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2016; pp. 1741–1745. ISBN 9781119296126. [Google Scholar]
- Kuroda, D.; Kawasaki, H.; Yamamoto, A.; Hiromoto, S.; Hanawa, T. Mechanical Properties and Microstructures of New Ti–Fe–Ta and Ti–Fe–Ta–Zr System Alloys. Mater. Sci. Eng. C Mater. Biol. Appl. 2005, 25, 312–320. [Google Scholar] [CrossRef]
- El Kadiri, H.; Wang, L.; Ozkan Gulsoy, H.; Suri, P.; Park, S.J.; Hammi, Y.; German, R.M. Development of a Ti-Based Alloy: Design and Experiment. JOM 2009, 61, 60–66. [Google Scholar] [CrossRef]
- Niinomi, M.; Liu, Y.; Nakai, M.; Liu, H.; Li, H. Biomedical Titanium Alloys with Young’s Moduli Close to That of Cortical Bone. Regen. Biomater. 2016, 3, 173–185. [Google Scholar] [CrossRef]
- Liu, H.; Niinomi, M.; Nakai, M.; Hieda, J.; Cho, K. Deformation Induced Changeable Young’s Modulus in Ternary Ti-Cr-O Alloys for Spinal Fixation Applications. In PRICM; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2013; pp. 1635–1641. ISBN 9781118792148. [Google Scholar]
- Jones, N.G.; Vorontsov, V.A.; Dye, D. The Behaviour of Gum Metal (Ti-36Nb-2Ta-3Zr-0.3 O wt.%) During Superelastic Cycling. In Proceedings of the 13th World Conference on Titanium; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2016; pp. 899–904. [Google Scholar]
- Ramarolahy, A.; Castany, P.; Prima, F.; Laheurte, P.; Péron, I.; Gloriant, T. Microstructure and Mechanical Behavior of Superelastic Ti–24Nb–0.5O and Ti–24Nb–0.5N Biomedical Alloys. J. Mech. Behav. Biomed. Mater. 2012, 9, 83–90. [Google Scholar] [CrossRef]
- Silva, D.G.; de Salvo, J.G.J.; Rodrigues Henriques, V.A. Microstructure Evolution during the Sintering of Blended Elemental Ti-23Nb-0.7Ta-2Zr-1.2O Gum Metal Alloy. In Proceedings of the SAE Technical Paper Series, SAE International: 400 Commonwealth Drive, Warrendale, PA, USA, 26 March 2021. [Google Scholar]
- Gordin, D.M.; Ion, R.; Vasilescu, C.; Drob, S.I.; Cimpean, A.; Gloriant, T. Potentiality of the “Gum Metal” Titanium-Based Alloy for Biomedical Applications. Mater. Sci. Eng. C Mater. Biol. Appl. 2014, 44, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.K.; Gustavson, L.J.; Dumbleton, J.H. Microstructure and Properties of a New Beta Titanium Alloy, Ti-12Mo-6Zr-2Fe, Developed for Surgical Implants. In Medical Applications of Titanium and Its Alloys: The Material and Biological Issues; ASTM International: West Conshohocken, PA, USA, 2009; pp. 76–87. ISBN 9780803120105. [Google Scholar]
- Civjan, S.; Huget, E.F.; DeSimon, L.B. Potential Applications of Certain Nickel-Titanium (Nitinol) Alloys. J. Dent. Res. 1975, 54, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Niinomi, M.; Nakai, M. Titanium-Based Biomaterials for Preventing Stress Shielding between Implant Devices and Bone. Int. J. Biomater. 2011, 2011, 836587. [Google Scholar] [CrossRef] [PubMed]
- Mahmud, A.; Huynh, T.; Zhou, L.; Hyer, H.; Mehta, A.; Imholte, D.D.; Woolstenhulme, N.E.; Wachs, D.M.; Sohn, Y. Mechanical Behavior Assessment of Ti-6Al-4V ELI Alloy Produced by Laser Powder Bed Fusion. Metals 2021, 11, 1671. [Google Scholar] [CrossRef]
- Afonso, C.R.M.; Aleixo, G.T.; Ramirez, A.J.; Caram, R. Influence of Cooling Rate on Microstructure of Ti–Nb Alloy for Orthopedic Implants. Mater. Sci. Eng. C Mater. Biol. Appl. 2007, 27, 908–913. [Google Scholar] [CrossRef]
- Ahmed, T.; Rack, H.J. Phase Transformations during Cooling in A+β Titanium Alloys. Materials Science and Engineering: A 1998, 243, 206–211. [Google Scholar] [CrossRef]
- Oh, J.-M.; Lim, J.-W.; Lee, B.-G.; Suh, C.-Y.; Cho, S.-W.; Lee, S.-W.; Choi, G.-S. Grain Refinement and Hardness Increase of Titanium via Trace Element Addition. Mater. Trans. 2010, 51, 2009–2012. [Google Scholar] [CrossRef]
- Simbi, D.J.; Scully, J.C. The Effect of Residual Interstitial Elements and Iron on Mechanical Properties of Commercially Pure Titanium. Mater. Lett. 1996, 26, 35–39. [Google Scholar] [CrossRef]
- Rooy, E.L.; Handbook, A. Volume 2: Properties and Selection: Nonferrous Alloys and Special-Purpose Materials; ASM International: Almere, The Netherlands, 1992. [Google Scholar]
- Yumak, N.; Aslantaş, K. A Review on Heat Treatment Efficiency in Metastable β Titanium Alloys: The Role of Treatment Process and Parameters. J. Mater. Res. Technol. 2020, 9, 15360–15380. [Google Scholar] [CrossRef]
- Semiatin, S.L.; Brown, T.M.; Goff, T.A.; Fagin, P.N.; Turner, R.E.; Murry, J.M.; Barker, D.R.; Miller, J.D.; Zhang, F. Diffusion Coefficients for Modeling the Heat Treatment of Ti-6Al-4V. Metall. Mater. Trans. A 2004, 35, 3015–3018. [Google Scholar] [CrossRef]
- Omoniyi, P.O.; Akinlabi, E.T.; Mahamood, R.M. Heat Treatments of Ti6Al4V Alloys for Industrial Applications: An Overview. IOP Conf. Ser. Mater. Sci. Eng. 2021, 1107, 012094. [Google Scholar] [CrossRef]
- Mahardika, M.; Akbar, F. Baroto Neutron Radiography and Tomography Investigations on the Porosity of the As-Cast Titanium Femoral Stem. IOP Conf. Ser. Mater. Sci. Eng. 2017, 172, 012057. [Google Scholar]
- Prayoga, B.T.; Dharmastiti, R.; Akbar, F. Suyitno Microstructural Characterization, Defect and Hardness of Titanium Femoral Knee Joint Produced Using Vertical Centrifugal Investment Casting. J. Mech. Sci. Technol. 2018, 32, 149–156. [Google Scholar] [CrossRef]
- Nakajima, H.; Okabe, T. Titanium in Dentistry Development and Research in the USA. Dent. Mater. J. 1996, 15, 77–90. [Google Scholar] [CrossRef]
- Menani, L.R.; Ribeiro, R.F.; de Almeida, R.P. Tensile Bond Strength of Cast Commercially Pure Titanium and Cast Gold-Alloy Posts and Cores Cemented with Two Luting Agents. J. Prosthet. Dent. 2008, 99, 141–147. [Google Scholar] [CrossRef]
- Gómez-Polo, M.; Llidó, B.; Rivero, A.; Del Río, J.; Celemín, A. A 10-Year Retrospective Study of the Survival Rate of Teeth Restored with Metal Prefabricated Posts versus Cast Metal Posts and Cores. J. Dent. 2010, 38, 916–920. [Google Scholar] [CrossRef]
- Saudi, A.U.; Wibisono, M.; Rianti, W.; Triwibowo, B.; Damisih, D.; Setyadi, I.; Gustiono, D.; Nurlina, N.; Kozin, M.; Jujur, I.N. Evaluation of Ti-6Al-7Nb Femoral Stem Fabricated by Centrifugal Investment Casting Using Fatigue Test. In AIP Conference Proceedings; AIP Publishing: Melville, NY, USA, 2022. [Google Scholar]
- Grivas, T.B.; Savvidou, O.D.; Psarakis, S.A.; Bernard, P.-F.; Triantafyllopoulos, G.; Kovanis, I.; Alexandropoulos, P. Neck Fracture of a Cementless Forged Titanium Alloy Femoral Stem Following Total Hip Arthroplasty: A Case Report and Review of the Literature. J. Med. Case Rep. 2007, 1, 174. [Google Scholar] [CrossRef]
- Semilitsch, M.; Willert, H.G. Properties of Implant Alloys for Artificial Hip Joints. Med. Biol. Eng. Comput. 1980, 18, 511–520. [Google Scholar] [CrossRef]
- Morgan-Hough, C.V.J.; Tavakkolizadeh, A.; Purkayastha, S. Fatigue Failure of the Femoral Component of a Cementless Total Hip Arthroplasty. J. Arthroplasty 2004, 19, 658–660. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.C.; Li, Y.J.; Tzou, G.Y. Study of the Titanium Alloy Deformation Behavior in Equal Channel Angular Extrusion. Key Eng. Mater. 2007, 345–346, 177–180. [Google Scholar] [CrossRef]
- Kent, D.; Wang, G.; Yu, Z.; Ma, X.; Dargusch, M. Strength Enhancement of a Biomedical Titanium Alloy through a Modified Accumulative Roll Bonding Technique. J. Mech. Behav. Biomed. Mater. 2011, 4, 405–416. [Google Scholar] [CrossRef] [PubMed]
- Lü, Z.D.; Zhang, C.J.; Feng, H.; Zhang, S.Z.; Han, J.C.; Jia, Y.; Du, Z.X.; Chen, Y.Y. Effect of Heat Treatment on Microstructure and Tensile Properties of 2 Vol.% TiCp/near-β Ti Composite Processed by Isothermal Multidirectional Forging. Mater. Sci. Eng. A Struct. Mater. 2019, 761, 138064. [Google Scholar] [CrossRef]
- Pachla, W.; Kulczyk, M.; Sus-Ryszkowska, M.; Mazur, A.; Kurzydlowski, K.J. Nanocrystalline Titanium Produced by Hydrostatic Extrusion. J. Mater. Process. Technol. 2008, 205, 173–182. [Google Scholar] [CrossRef]
- Zareena, A.R.; Veldhuis, S.C. Tool Wear Mechanisms and Tool Life Enhancement in Ultra-Precision Machining of Titanium. J. Mater. Process. Technol. 2012, 212, 560–570. [Google Scholar] [CrossRef]
- Madyira, D.M.; Laubscher, R.F.; van Rensburg, N.J.; Henning, P.F.J. High Speed Machining Induced Residual Stresses in Grade 5 Titanium Alloy. Proc. Inst. Mech. Eng. L J. Mater. Des. Appl. 2013, 227, 208–215. [Google Scholar] [CrossRef]
- Pan, Z.; Liang, S.Y.; Garmestani, H. Finite Element Simulation of Residual Stress in Machining of Ti-6Al-4V with a Microstructural Consideration. Proc. Inst. Mech. Eng. Pt. B J. Eng. Manuf. 2019, 233, 1103–1111. [Google Scholar] [CrossRef]
- Murr, L.E.; Amato, K.N.; Li, S.J.; Tian, Y.X.; Cheng, X.Y.; Gaytan, S.M.; Martinez, E.; Shindo, P.W.; Medina, F.; Wicker, R.B. Microstructure and Mechanical Properties of Open-Cellular Biomaterials Prototypes for Total Knee Replacement Implants Fabricated by Electron Beam Melting. J. Mech. Behav. Biomed. Mater. 2011, 4, 1396–1411. [Google Scholar] [CrossRef]
- Zhao, S.; Li, S.J.; Hou, W.T.; Hao, Y.L.; Yang, R.; Murr, L.E. Microstructure and Mechanical Properties of Open Cellular Ti–6Al–4V Prototypes Fabricated by Electron Beam Melting for Biomedical Applications. Mater. Technol. 2016, 31, 98–107. [Google Scholar] [CrossRef]
- Del Guercio, G.; Galati, M.; Saboori, A.; Fino, P.; Iuliano, L. Microstructure and Mechanical Performance of Ti–6Al–4V Lattice Structures Manufactured via Electron Beam Melting (EBM): A Review. Acta Metall. Sin. (Engl. Lett.) 2020, 33, 183–203. [Google Scholar] [CrossRef]
- Khomutov, M.; Potapkin, P.; Cheverikin, V.; Petrovskiy, P.; Travyanov, A.; Logachev, I.; Sova, A.; Smurov, I. Effect of Hot Isostatic Pressing on Structure and Properties of Intermetallic NiAl–Cr–Mo Alloy Produced by Selective Laser Melting. Intermetallics (Barking) 2020, 120, 106766. [Google Scholar] [CrossRef]
- Tammas-Williams, S.; Withers, P.J.; Todd, I.; Prangnell, P.B. The Effectiveness of Hot Isostatic Pressing for Closing Porosity in Titanium Parts Manufactured by Selective Electron Beam Melting. Metall. Mater. Trans. A 2016, 47, 1939–1946. [Google Scholar] [CrossRef]
- Ramamurthy, A.; Sivaramakrishnan, R.; Muthuramalingam, T.; Venugopal, S. Performance Analysis of Wire Electrodes on Machining Ti-6Al-4V Alloy Using Electrical Discharge Machining Process. Mach. Sci. Technol. 2015, 19, 577–592. [Google Scholar] [CrossRef]
- Hasçalık, A.; Çaydaş, U. Electrical Discharge Machining of Titanium Alloy (Ti–6Al–4V). Appl. Surf. Sci. 2007, 253, 9007–9016. [Google Scholar] [CrossRef]
- Vasanth, S.; Muthuramalingam, T.; Vinothkumar, P.; Geethapriyan, T.; Murali, G. Performance Analysis of Process Parameters on Machining Titanium (Ti-6Al-4V) Alloy Using Abrasive Water Jet Machining Process. Procedia CIRP 2016, 46, 139–142. [Google Scholar] [CrossRef]
- Hascalik, A.; Çaydaş, U.; Gürün, H. Effect of Traverse Speed on Abrasive Waterjet Machining of Ti–6Al–4V Alloy. Mater. Eng. 2007, 28, 1953–1957. [Google Scholar] [CrossRef]
- Muthuramalingam, T.; Akash, R.; Krishnan, S.; Phan, N.H.; Pi, V.N.; Elsheikh, A.H. Surface Quality Measures Analysis and Optimization on Machining Titanium Alloy Using CO2 Based Laser Beam Drilling Process. J. Manuf. Process. 2021, 62, 1–6. [Google Scholar] [CrossRef]
- Muthuramalingam, T.; Moiduddin, K.; Akash, R.; Krishnan, S.; Hammad Mian, S.; Ameen, W.; Alkhalefah, H. Influence of Process Parameters on Dimensional Accuracy of Machined Titanium (Ti-6Al-4V) Alloy in Laser Beam Machining Process. Opt. Laser Technol. 2020, 132, 106494. [Google Scholar] [CrossRef]
- Singh, R.; Khamba, J.S. Ultrasonic Machining of Titanium and Its Alloys: A Review. J. Mater. Process. Technol. 2006, 173, 125–135. [Google Scholar] [CrossRef]
- Kumar, J.; Khamba, J.S.; Mohapatra, S.K. An Investigation into the Machining Characteristics of Titanium Using Ultrasonic Machining. Int. J. Mach. Mach. Mater. 2008, 3, 143. [Google Scholar] [CrossRef]
- Yang, X.; Richard Liu, C. Machining Titanium and Its Alloys. Mach. Sci. Technol. 1999, 3, 107–139. [Google Scholar] [CrossRef]
- Dewidar, M.M.; Yoon, H.-C.; Lim, J.K. Mechanical Properties of Metals for Biomedical Applications Using Powder Metallurgy Process: A Review. Met. Mater. Int. 2006, 12, 193–206. [Google Scholar] [CrossRef]
- Zhang, L.-C.; Liu, Y. Additive Manufacturing of Titanium Alloys for Biomedical Applications. In Additive Manufacturing of Emerging Materials; Springer International Publishing: Cham, Switzerland, 2019; pp. 179–196. ISBN 9783319917122. [Google Scholar]
- Bolzoni, L.; Ruiz-Navas, E.M.; Gordo, E. Feasibility Study of the Production of Biomedical Ti–6Al–4V Alloy by Powder Metallurgy. Mater. Sci. Eng. C Mater. Biol. Appl. 2015, 49, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Manne, P.K.; Shravan Kumar, N.; Buddi, T.; Lakshmi, A.A.; Subbiah, R. Powder Metallurgy Techniques for Titanium Alloys-A Review. E3S Web Conf. 2020, 184, 01045. [Google Scholar] [CrossRef]
- Wen, M.; Wen, C.; Hodgson, P.; Li, Y. Fabrication of Ti–Nb–Ag Alloy via Powder Metallurgy for Biomedical Applications. Mater. Eng. 2014, 56, 629–634. [Google Scholar] [CrossRef]
- Liu, Y.; Li, K.; Luo, T.; Song, M.; Wu, H.; Xiao, J.; Tan, Y.; Cheng, M.; Chen, B.; Niu, X.; et al. Powder Metallurgical Low-Modulus Ti-Mg Alloys for Biomedical Applications. Mater. Sci. Eng. C Mater. Biol. Appl. 2015, 56, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Bolzoni, L.; Yang, F. Development of Cu-Bearing Powder Metallurgy Ti Alloys for Biomedical Applications. J. Mech. Behav. Biomed. Mater. 2019, 97, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Lario, J.; Vicente, Á.; Amigó, V. Evolution of the Microstructure and Mechanical Properties of a Ti35Nb2Sn Alloy Post-Processed by Hot Isostatic Pressing for Biomedical Applications. Metals 2021, 11, 1027. [Google Scholar] [CrossRef]
- Abdullah, Z.; Razali, R.; Subuki, I.; Omar, M.A.; Ismail, M.H. An Overview of Powder Metallurgy (PM) Method for Porous Nickel Titanium Shape Memory Alloy (SMA). Adv. Mater. Res. 2016, 1133, 269–274. [Google Scholar] [CrossRef]
- Zhang, L.-C.; Liu, Y.; Li, S.; Hao, Y. Additive Manufacturing of Titanium Alloys by Electron Beam Melting: A Review. Adv. Eng. Mater. 2018, 20, 1700842. [Google Scholar] [CrossRef]
- Munir, K.; Biesiekierski, A.; Wen, C.; Li, Y. Selective Laser Melting in Biomedical Manufacturing. In Metallic Biomaterials Processing and Medical Device Manufacturing; Elsevier: Amsterdam, The Netherlands, 2020; pp. 235–269. ISBN 9780081029657. [Google Scholar]
- Mishurova, T.; Cabeza, S.; Artzt, K.; Haubrich, J.; Klaus, M.; Genzel, C.; Requena, G.; Bruno, G. An assessment of subsurface residual stress analysis in SLM Ti-6Al-4V. Materials 2017, 10, 348. [Google Scholar] [CrossRef]
- Denlinger, E.R.; Heigel, J.C.; Michaleris, P.; Palmer, T.A. Effect of Inter-Layer Dwell Time on Distortion and Residual Stress in Additive Manufacturing of Titanium and Nickel Alloys. J. Mater. Process. Technol. 2015, 215, 123–131. [Google Scholar] [CrossRef]
- Namavar, F.; Sabirianov, R.; Marton, D.; Rubinstein, A.; Garvin, K. Biocompatibility of Titanium. 1 February 2012; Volume 2012, p. C1.148. Available online: https://ui.adsabs.harvard.edu/ (accessed on 15 October 2023).
- Bhola, R.; Bhola, S.M.; Mishra, B.; Olson, D.L. Corrosion in Titanium Dental Implants/Prostheses—A Review. Trends Biomater. Artif. Organs 2011, 25, 34–46. [Google Scholar]
- Barberi, J.; Spriano, S. Titanium and Protein Adsorption: An Overview of Mechanisms and Effects of Surface Features. Materials 2021, 14, 1590. [Google Scholar] [CrossRef] [PubMed]
- Geetha, M.; Kamachi Mudali, U.; Gogia, A.K.; Asokamani, R.; Raj, B. Influence of Microstructure and Alloying Elements on Corrosion Behavior of Ti–13Nb–13Zr Alloy. Corros. Sci. 2004, 46, 877–892. [Google Scholar] [CrossRef]
- Chen, M.; Zhang, E.; Zhang, L. Microstructure, Mechanical Properties, Bio-Corrosion Properties and Antibacterial Properties of Ti-Ag Sintered Alloys. Mater. Sci. Eng. C Mater. Biol. Appl. 2016, 62, 350–360. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Liu, Y.; Pang, S.; Liaw, P.K.; Zhang, T. Bio-Corrosion Behavior and in Vitro Biocompatibility of Equimolar TiZrHfNbTa High-Entropy Alloy. Intermetallics (Barking) 2020, 124, 106845. [Google Scholar] [CrossRef]
- Niu, J.; Guo, Y.; Li, K.; Liu, W.; Dan, Z.; Sun, Z.; Chang, H.; Zhou, L. Improved Mechanical, Bio-Corrosion Properties and in Vitro Cell Responses of Ti-Fe Alloys as Candidate Dental Implants. Mater. Sci. Eng. C Mater. Biol. Appl. 2021, 122, 111917. [Google Scholar] [CrossRef]
- Manoj, A.; Kasar, A.K.; Menezes, P.L. Tribocorrosion of Porous Titanium Used in Biomedical Applications. J. Bio- Tribo-Corros. 2019, 5, 1–16. [Google Scholar] [CrossRef]
- Hacisalihoglu, I.; Samancioglu, A.; Yildiz, F.; Purcek, G.; Alsaran, A. Tribocorrosion Properties of Different Type Titanium Alloys in Simulated Body Fluid. Wear 2015, 332–333, 679–686. [Google Scholar] [CrossRef]
- Diomidis, N.; Mischler, S.; More, N.S.; Roy, M.; Paul, S.N. Fretting-Corrosion Behavior of β Titanium Alloys in Simulated Synovial Fluid. Wear 2011, 271, 1093–1102. [Google Scholar] [CrossRef]
- Kumar, S.; Sankara Narayanan, T.S.N.; Ganesh Sundara Raman, S.; Seshadri, S.K. Evaluation of Fretting Corrosion Behaviour of CP-Ti for Orthopaedic Implant Applications. Tribol. Int. 2010, 43, 1245–1252. [Google Scholar] [CrossRef]
- Souza, M.E.P.; Lima, L.; Lima, C.R.P.; Zavaglia, C.A.C.; Freire, C.M.A. Effects of PH on the Electrochemical Behaviour of Titanium Alloys for Implant Applications. J. Mater. Sci. Mater. Med. 2009, 20, 549–552. [Google Scholar] [CrossRef] [PubMed]
- Manivasagam, G.; Mudali, U.K.; Asokamani, R.; Raj, B. Corrosion and Microstructural Aspects of Titanium and Its Alloys as Orthopaedic Devices. Corros. Rev. 2003, 21, 125–160. [Google Scholar] [CrossRef]
- Woodman, J.L.; Jacobs, J.J.; Galante, J.O.; Urban, R.M. Metal Ion Release from Titanium-Based Prosthetic Segmental Replacements of Long Bones in Baboons: A Long-Term Study. J. Orthop. Res. 1984, 1, 421–430. [Google Scholar] [CrossRef] [PubMed]
- Pitchi, C.S.; Priyadarshini, A.; Sana, G.; Narala, S.K.R. A Review on Alloy Composition and Synthesis of β-Titanium Alloys for Biomedical Applications. Mater. Today 2020, 26, 3297–3304. [Google Scholar] [CrossRef]
- Okulov, I.V.; Volegov, A.S.; Attar, H.; Bönisch, M.; Ehtemam-Haghighi, S.; Calin, M.; Eckert, J. Composition Optimization of Low Modulus and High-Strength TiNb-Based Alloys for Biomedical Applications. J. Mech. Behav. Biomed. Mater. 2017, 65, 866–871. [Google Scholar] [CrossRef] [PubMed]
- Markowska-Szczupak, A.; Endo-Kimura, M.; Paszkiewicz, O.; Kowalska, E. Are titania photocatalysts and titanium implants safe? Review on the toxicity of titanium compounds. Nanomaterials 2020, 10, 2065. [Google Scholar] [CrossRef]
- Block, M.S. Dental Implants: The Last 100 Years. J. Oral Maxillofac. Surg. 2018, 76, 11–26. [Google Scholar] [CrossRef]
- Espinoza-Montero, P.J.; Montero-Jiménez, M.; Fernández, L.; Paz, J.L.; Piñeiros, J.L.; Ceballos, S.M. In Vitro Wearing Away of Orthodontic Brackets and Wires in Different Conditions: A Review. Heliyon 2022, 8, e10560. [Google Scholar] [CrossRef]
- Donley, T.G.; Gillette, W.B. Titanium Endosseous Implant-Soft Tissue Interface: A Literature Review. J. Periodontol. 1991, 62, 153–160. [Google Scholar] [CrossRef]
- Nergiz, I.; Schmage, P.; Ozcan, M.; Platzer, U. Effect of Length and Diameter of Tapered Posts on the Retention. J. Oral Rehabil. 2002, 29, 28–34. [Google Scholar] [CrossRef]
- Lambjerg-Hansen, H.; Asmussen, E. Mechanical Properties of Endodontic Posts. J. Oral Rehabil. 2008, 24, 882–887. [Google Scholar] [CrossRef]
- Burstone, C.J.; Goldberg, A.J. Beta Titanium: A New Orthodontic Alloy. Am. J. Orthod. 1980, 77, 121–132. [Google Scholar] [CrossRef] [PubMed]
- Brantley, W.A. Evolution, Clinical Applications, and Prospects of Nickel-Titanium Alloys for Orthodontic Purposes. J. World Fed. Orthod. 2020, 9, S19–S26. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, Y.; Komatsu, H.; Murata, Y.; Tanaka, T.; Sano, H. A Newly Designed Automatic PH-Cycling System to Simulate Daily PH Fluctuations. Dent. Mater. J. 2006, 25, 280–285. [Google Scholar] [CrossRef]
- Roehling, S.; Astasov-Frauenhoffer, M.; Hauser-Gerspach, I.; Braissant, O.; Woelfler, H.; Waltimo, T.; Kniha, H.; Gahlert, M. In Vitro Biofilm Formation on Titanium and Zirconia Implant Surfaces. J. Periodontol. 2017, 88, 298–307. [Google Scholar] [CrossRef]
- Bürgers, R.; Gerlach, T.; Hahnel, S.; Schwarz, F.; Handel, G.; Gosau, M. In Vivo and in Vitro Biofilm Formation on Two Different Titanium Implant Surfaces. Clin. Oral Implants Res. 2010, 21, 156–164. [Google Scholar] [CrossRef]
- Martínez-Hernández, M.; Olivares-Navarrete, R.; Almaguer-Flores, A. Influence of the Periodontal Status on the Initial-Biofilm Formation on Titanium Surfaces. Clin. Implant Dent. Relat. Res. 2016, 18, 174–181. [Google Scholar] [CrossRef]
- Haraldson, T.; Karlsson, U.; Carlsson, G.E. Bite Force and Oral Function in Complete Denture Wearers. J. Oral Rehabil. 1979, 6, 41–48. [Google Scholar] [CrossRef]
- Haraldson, T.; Carlsson, G.E. Bite Force and Oral Function in Patients with Osseointegrated Oral Implants. Scand. J. Dent. Res. 1977, 85, 200–208. [Google Scholar] [CrossRef]
- van Eijden, T.M. Three-Dimensional Analyses of Human Bite-Force Magnitude and Moment. Arch. Oral Biol. 1991, 36, 535–539. [Google Scholar] [CrossRef]
- Moraschini, V.; Poubel, L.A.D.C.; Ferreira, V.F.; Barboza, E.D.S.P. Evaluation of Survival and Success Rates of Dental Implants Reported in Longitudinal Studies with a Follow-up Period of at Least 10 Years: A Systematic Review. Int. J. Oral Maxillofac. Surg. 2015, 44, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Messias, A.; Nicolau, P.; Guerra, F. Titanium Dental Implants with Different Collar Design and Surface Modifications: A Systematic Review on Survival Rates and Marginal Bone Levels. Clin. Oral Implants Res. 2019, 30, 20–48. [Google Scholar] [CrossRef] [PubMed]
- Madhukar, S.; Nakshatram, S.; Naik, R.P.; Butty, P. Review on Use of Titanium and Its Alloys as Implants in Dental Applications. Int. J. Curr. Eng. Technol. 2020, 10, 513–517. [Google Scholar] [CrossRef]
- Altuna, P.; Lucas-Taulé, E.; Gargallo-Albiol, J.; Figueras-Álvarez, O.; Hernández-Alfaro, F.; Nart, J. Clinical Evidence on Titanium-Zirconium Dental Implants: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Surg. 2016, 45, 842–850. [Google Scholar] [CrossRef] [PubMed]
- Sales, P.H.D.H.; Barros, A.W.P.; de Oliveira-Neto, O.B.; de Lima, F.J.C.; Carvalho, A.D.A.T.; Leão, J.C. Do Zirconia Dental Implants Present Better Clinical Results than Titanium Dental Implants? A Systematic Review and Meta-Analysis. J. Stomatol. Oral Maxillofac. Surg. 2023, 124, 101324. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Menini, M.; Santori, G.; Rakic, M.; Sculean, A.; Pesce, P. Titanium Abutment Surface Modifications and Peri-Implant Tissue Behavior: A Systematic Review and Meta-Analysis. Clin. Oral Investig. 2020, 24, 1113–1124. [Google Scholar] [CrossRef]
- Haugen, H.J.; Chen, H. Is There a Better Biomaterial for Dental Implants than Titanium?—A Review and Meta-Study Analysis. J. Funct. Biomater. 2022, 13, 46. [Google Scholar] [CrossRef]
- Chang, H.-P.; Tseng, Y.-C. A Novel β-Titanium Alloy Orthodontic Wire. Kaohsiung J. Med. Sci. 2018, 34, 202–206. [Google Scholar] [CrossRef]
- Castro, S.M.; Ponces, M.J.; Lopes, J.D.; Vasconcelos, M.; Pollmann, M.C.F. Orthodontic Wires and Its Corrosion—The Specific Case of Stainless Steel and Beta-Titanium. J. Dent. Sci. 2015, 10, 1–7. [Google Scholar] [CrossRef]
- Kolli, R.; Devaraj, A. A Review of Metastable Beta Titanium Alloys. Metals 2018, 8, 506. [Google Scholar] [CrossRef]
- Chahine, G.; Koike, M.; Okabe, T.; Smith, P.; Kovacevic, R. The Design and Production of Ti-6Al-4V ELI Customized Dental Implants. JOM (1989) 2008, 60, 50–55. [Google Scholar] [CrossRef]
- Chen, X.; Shah, K.; Dong, S.; Peterson, L.; La Plante, E.C.; Sant, G. Elucidating the corrosion-related degradation mechanisms of a Ti-6Al-4V dental implant. Dent. Mater. 2020, 36, 431–441. [Google Scholar] [CrossRef] [PubMed]
- Berbel, L.O.; Banczek, E.D.P.; Karoussis, I.K.; Kotsakis, G.A.; Costa, I. Determinants of Corrosion Resistance of Ti-6Al-4V Alloy Dental Implants in an In Vitro Model of Peri-Implant Inflammation. PLoS ONE 2019, 14, e0217671. [Google Scholar]
- Xiong, Y.; Wang, W.; Gao, R.; Zhang, H.; Dong, L.; Qin, J.; Wang, B.; Jia, W.; Li, X. Fatigue Behavior and Osseointegration of Porous Ti-6Al-4V Scaffolds with Dense Core for Dental Application. Mater. Des. 2020, 195, 108994. [Google Scholar] [CrossRef]
- Cai, Z.; Bunce, N.; Nunn, M.E.; Okabe, T. Porcelain Adherence to Dental Cast CP Titanium: Effects of Surface Modifications. Biomaterials 2001, 22, 979–986. [Google Scholar] [CrossRef]
- McCracken, M. Dental Implant Materials: Commercially Pure Titanium and Titanium Alloys. J. Prosthodont. 1999, 8, 40–43. [Google Scholar] [CrossRef]
- Souza, J.C.M.; Henriques, B.; Ariza, E.; Martinelli, A.E.; Nascimento, R.M.; Silva, F.S.; Rocha, L.A.; Celis, J.-P. Mechanical and Chemical Analyses across Dental Porcelain Fused to CP Titanium or Ti6Al4V. Mater. Sci. Eng. C Mater. Biol. Appl. 2014, 37, 76–83. [Google Scholar] [CrossRef]
- Ohkubo, C.; Hanatani, S.; Hosoi, T. Present Status of Titanium Removable Dentures—A Review of the Literature. J. Oral Rehabil. 2008, 35, 706–714. [Google Scholar] [CrossRef]
- Jensen, O.T.; Jansen, C.E.; Seo, Y.; Yellich, G. Guided Nitinol-Retained (Smileloc) Single-Tooth Dental Restorations. Oral Maxillofac. Surg. Clin. N. Am. 2019, 31, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Cutright, D.E.; Bhaskar, S.N.; Perez, B.; Johnson, R.M.; Cowan, G.S., Jr. Tissue Reaction to Nitinol Wire Alloy. Oral Surg. Oral Med. Oral Pathol. 1973, 35, 578–584. [Google Scholar] [CrossRef]
- Development of Novel Implant Abutments Using the Shape Memory Alloy Nitinol: Preliminary Results. J. Prosthet. Dent. 2010, 104, 181. [CrossRef]
- Castagnini, F.; Bordini, B.; Stea, S.; Calderoni, P.P.; Masetti, C.; Busanelli, L. Highly Porous Titanium Cup in Cementless Total Hip Arthroplasty: Registry Results at Eight Years. Int. Orthop. 2019, 43, 1815–1821. [Google Scholar] [CrossRef] [PubMed]
- Campanelli, L.C. A Review on the Recent Advances Concerning the Fatigue Performance of Titanium Alloys for Orthopedic Applications. J. Mater. Res. 2021, 36, 151–165. [Google Scholar] [CrossRef]
- Healy, W.L.; Tilzey, J.F.; Iorio, R.; Specht, L.M.; Sharma, S. Prospective, Randomized Comparison of Cobalt-Chrome and Titanium Trilock Femoral Stems. J. Arthroplast. 2009, 24, 831–836. [Google Scholar] [CrossRef] [PubMed]
- Bridgeman, J.T.; Marker, V.A.; Hummel, S.K.; Benson, B.W.; Pace, L.L. Comparison of Titanium and Cobalt-Chromium Removable Partial Denture Clasps. J. Prosthet. Dent. 1997, 78, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Morwood, M.P.; Garrigues, G.E. Shoulder Arthroplasty in the Patient with Metal Hypersensitivity. J. Shoulder Elbow Surg. 2015, 24, 1156–1164. [Google Scholar] [CrossRef]
- Little, C.P.; Graham, A.J.; Carr, A.J. Total Elbow Arthroplasty. J. Bone Jt. Surg. Br. 2005, 87-B, 437–444. [Google Scholar] [CrossRef]
- Radmer, S.; Andresen, R.; Sparmann, M. Total Wrist Arthroplasty in Patients with Rheumatoid Arthritis. J. Hand Surg. Am. 2003, 28, 789–794. [Google Scholar] [CrossRef]
- Semlitsch, M. Titanium Alloys for Hip Joint Replacements. Clin. Mater. 1987, 2, 1–13. [Google Scholar] [CrossRef]
- King, S.W.; Royeca, J.M.; Cunningham, C.M.; Madegowda, R.; Sha, S.; Pandit, H. Metal Hypersensitivity in Total Knee Arthroplasty. J. Arthrosc. Jt. Surg. 2020, 7, 184–188. [Google Scholar] [CrossRef]
- Easley, M.E.; Vertullo, C.J.; Urban, W.C.; Nunley, J.A. Total Ankle Arthroplasty. J. Am. Acad. Orthop. Surg. 2002, 10, 157–167. [Google Scholar] [CrossRef]
- Miller, P.D.; Holladay, J.W. Friction and Wear Properties of Titanium. Wear 1958, 2, 133–140. [Google Scholar] [CrossRef]
- Marshall, A.D.; Mokris, J.G.; Reitman, R.D.; Dandar, A.; Mauerhan, D.R. Cementless Titanium Tapered-Wedge Femoral Stem: 10- to 15-Year Follow-Up. J. Arthroplasty 2004, 19, 546–552. [Google Scholar] [CrossRef]
- De Meo, F.; Cacciola, G.; Bellotti, V.; Bruschetta, A.; Cavaliere, P. Trabecular Titanium Acetabular Cups in Hip Revision Surgery: Mid-Term Clinical and Radiological Outcomes. Hip Int. 2018, 28, 61–65. [Google Scholar] [CrossRef]
- Hell, A.K.; Campbell, R.M.; Hefti, F. The Vertical Expandable Prosthetic Titanium Rib Implant for the Treatment of Thoracic Insufficiency Syndrome Associated with Congenital and Neuromuscular Scoliosis in Young Children. J. Pediatr. Orthop. B 2005, 14, 287–293. [Google Scholar] [CrossRef]
- Blake, G.B.; MacFarlane, M.R.; Hinton, J.W. Titanium in Reconstructive Surgery of the Skull and Face. Br. J. Plast. Surg. 1990, 43, 528–535. [Google Scholar] [CrossRef]
- Zuo, W.; Yu, L.; Lin, J.; Yang, Y.; Fei, Q. Properties Improvement of Titanium Alloys Scaffolds in Bone Tissue Engineering: A Literature Review. Ann. Transl. Med. 2021, 9, 1259. [Google Scholar] [CrossRef]
- Liang, H.; Yang, Y.; Xie, D.; Li, L.; Mao, N.; Wang, C.; Tian, Z.; Jiang, Q.; Shen, L. Trabecular-like Ti-6Al-4V Scaffolds for Orthopedic: Fabrication by Selective Laser Melting and in Vitro Biocompatibility. J. Mater. Sci. Technol. 2019, 35, 1284–1297. [Google Scholar] [CrossRef]
- Aufa, A.N.; Hassan, M.Z.; Ismail, Z. Recent Advances in Ti-6Al-4V Additively Manufactured by Selective Laser Melting for Biomedical Implants: Prospect Development. J. Alloys Compd. 2022, 896, 163072. [Google Scholar] [CrossRef]
- Shen, X.; Shukla, P.; Subramaniyan, A.K.; Zammit, A.; Swanson, P.; Lawrence, J.; Fitzpatrick, M.E. Residual Stresses Induced by Laser Shock Peening in Orthopaedic Ti-6Al-7Nb Alloy. Opt. Laser Technol. 2020, 131, 106446. [Google Scholar] [CrossRef]
- Milošev, I.; Kosec, T.; Strehblow, H.-H. XPS and EIS Study of the Passive Film Formed on Orthopaedic Ti–6Al–7Nb Alloy in Hank’s Physiological Solution. Electrochim. Acta 2008, 53, 3547–3558. [Google Scholar] [CrossRef]
- Łyczkowska, E.; Szymczyk, P.; Dybała, B.; Chlebus, E. Chemical Polishing of Scaffolds Made of Ti–6Al–7Nb Alloy by Additive Manufacturing. Arch. Civ. Mech. Eng. 2014, 14, 586–594. [Google Scholar] [CrossRef]
- Jablokov, V.R.; Nutt, M.J.; Richelsoph, M.E.; Freese, H.L. The Application of Ti-15Mo Beta Titanium Alloy in High Strength Structural Orthopaedic Applications. In Titanium, Niobium, Zirconium, and Tantalum for Medical and Surgical Applications; ASTM International: West Conshohocken, PA, USA, 2008; pp. 1–18. ISBN 9780803134973. [Google Scholar]
- Oliveira, N.T.; Perrotti, V.; Palmieri, A.; Guastaldi, A.C.; Pellati, A.; Scapin, C.L.; Piattelli, A.; Carinci, F. In Vitro Analysis with Human Bone Marrow Stem Cells on Ti-15Mo Alloy for Dental and Orthopedic Implants Application. J. Osseointegr. 2011, 3, 10–16. [Google Scholar]
- Suresh, K.S.; Geetha, M.; Richard, C.; Landoulsi, J.; Ramasawmy, H.; Suwas, S.; Asokamani, R. Effect of Equal Channel Angular Extrusion on Wear and Corrosion Behavior of the Orthopedic Ti–13Nb–13Zr Alloy in Simulated Body Fluid. Mater. Sci. Eng. C Mater. Biol. Appl. 2012, 32, 763–771. [Google Scholar] [CrossRef]
- Cvijović-Alagić, I.; Cvijović, Z.; Mitrović, S.; Rakin, M.; Veljović, Đ.; Babić, M. Tribological Behaviour of Orthopaedic Ti-13Nb-13Zr and Ti-6Al-4V Alloys. Tribol. Lett. 2010, 40, 59–70. [Google Scholar] [CrossRef]
- Khan, M.A.; Williams, R.L.; Williams, D.F. The Corrosion Behaviour of Ti-6Al-4V, Ti-6Al-7Nb and Ti-13Nb-13Zr in Protein Solutions. Biomaterials 1999, 20, 631–637. [Google Scholar] [CrossRef]
- Albrektsson, T.; Becker, W.; Coli, P.; Jemt, T.; Mölne, J.; Sennerby, L. Bone Loss around Oral and Orthopedic Implants: An Immunologically Based Condition. Clin. Implant Dent. Relat. Res. 2019, 21, 786–795. [Google Scholar] [CrossRef]
- Albrektsson, T.; Chrcanovic, B.; Mölne, J.; Wennerberg, A. Foreign Body Reactions, Marginal Bone Loss and Allergies in Relation to Titanium Implants. Eur. J. Oral Implantol. 2018, 11 (Suppl. S1), S37–S46. [Google Scholar]
- Lin, C.W.; Ju, C.P.; Lin, J.H.C. A Comparison of the Fatigue Behavior of Cast Ti-7.5 Mo with Cp Titanium, Ti-6Al-4V and Ti-13Nb-13Zr Alloys. Biomaterials 2005, 26, 2899–2907. [Google Scholar] [CrossRef]
- Pelton, A.R.; Stöckel, D.; Duerig, T.W. Medical uses of nitinol. In Materials Science Forum; Trans Tech Publications Ltd.: Stafa-Zurich, Switzerland, 2000; Volume 327, pp. 63–70. [Google Scholar]
- Banovetz, J.M.; Sharp, R.; Probe, R.A.; Anglen, J.O. Titanium Plate Fixation: A Review of Implant Failures. J. Orthop. Trauma 1996, 10, 389–394. [Google Scholar] [CrossRef]
- Perren, S.M.; Regazzoni, P.; Fernandez, A.A. How to Choose between the Implant Materials Steel and Titanium in Orthopedic Trauma Surgery: Part 2—Biological Aspects. Acta Chir. Orthop. Traumatol. Cech. 2017, 84, 85–90. [Google Scholar] [CrossRef]
- Arens, S.; Schlegel, U.; Printzen, G.; Ziegler, W.J.; Perren, S.M.; Hansis, M. Influence of Materials for Fixation Implants on Local Infection. An Experimental Study of Steel versus Titanium DCP in Rabbits. J. Bone Jt. Surg. Br. 1996, 78, 647–651. [Google Scholar] [CrossRef]
- Vancleef, S.; Wesseling, M.; Duflou, J.R.; Nijs, S.; Jonkers, I.; Vander Sloten, J. Thin Patient-Specific Clavicle Fracture Fixation Plates Can Mechanically Outperform Commercial Plates: An in Silico Approach. J. Orthop. Res. 2022, 40, 1695–1706. [Google Scholar] [CrossRef]
- Kumazawa, R.; Watari, F.; Takashi, N.; Tanimura, Y.; Uo, M.; Totsuka, Y. Effects of Ti Ions and Particles on Neutrophil Function and Morphology. Biomaterials 2002, 23, 3757–3764. [Google Scholar] [CrossRef]
- Mohi Eldin, M.M.; Ali, A.M.A. Lumbar Transpedicular Implant Failure: A Clinical and Surgical Challenge and Its Radiological Assessment. Asian Spine J. 2014, 8, 281–297. [Google Scholar] [CrossRef]
- Szypryt, P.; Forward, D. The Use and Abuse of Locking Plates. Orthop. Trauma 2009, 23, 281–290. [Google Scholar] [CrossRef]
- Jost, B.; Spross, C.; Grehn, H.; Gerber, C. Locking Plate Fixation of Fractures of the Proximal Humerus: Analysis of Complications, Revision Strategies and Outcome. J. Shoulder Elbow Surg. 2013, 22, 542–549. [Google Scholar] [CrossRef]
- Disegi, J.A. Titanium Alloys for Fracture Fixation Implants. Injury 2000, 31 (Suppl. 4), 14–17. [Google Scholar] [CrossRef]
- Valiev, R.Z.; Semenova, I.P.; Latysh, V.V.; Rack, H.; Lowe, T.C.; Petruzelka, J.; Dluhos, L.; Hrusak, D.; Sochova, J. Nanostructured Titanium for Biomedical Applications. Adv. Eng. Mater. 2008, 10, B15–B17. [Google Scholar] [CrossRef]
- Krischak, G.D.; Gebhard, F.; Mohr, W.; Krivan, V.; Ignatius, A.; Beck, A.; Wachter, N.J.; Reuter, P.; Arand, M.; Kinzl, L.; et al. Difference in Metallic Wear Distribution Released from Commercially Pure Titanium Compared with Stainless Steel Plates. Arch. Orthop. Trauma Surg. 2004, 124, 104–113. [Google Scholar] [CrossRef]
- Koller, H.; Zenner, J.; Hempfing, A.; Ferraris, L.; Meier, O. Reinforcement of Lumbosacral Instrumentation Using S1-Pedicle Screws Combined with S2-Alar Screws. Oper. Orthop. Traumatol. 2013, 25, 294–314. [Google Scholar] [CrossRef]
- Fourney, D.R.; Abi-Said, D.; Lang, F.F.; McCutcheon, I.E.; Gokaslan, Z.L. Use of Pedicle Screw Fixation in the Management of Malignant Spinal Disease: Experience in 100 Consecutive Procedures. J. Neurosurg. Spine 2001, 94, 25–37. [Google Scholar] [CrossRef]
- Fukutake, K.; Wada, A.; Kamakura, D.; Nakamura, K.; Tsuge, S.; Hasegawa, K.; Takahashi, H. Evaluation of Percutaneous Pedicle Screw Fixation in Patients with Pyogenic Spondylitis of the Thoracolumbar Spine. Open J. Orthop. 2020, 10, 303–312. [Google Scholar] [CrossRef]
- Yamanaka, K.; Mori, M.; Yamazaki, K.; Kumagai, R.; Doita, M.; Chiba, A. Analysis of the Fracture Mechanism of Ti-6Al-4V Alloy Rods That Failed Clinically after Spinal Instrumentation Surgery. Spine 2015, 40, E767–E773. [Google Scholar] [CrossRef]
- Massaad, E.; Fatima, N.; Kiapour, A.; Hadzipasic, M.; Shankar, G.M.; Shin, J.H. Polyetheretherketone versus Titanium Cages for Posterior Lumbar Interbody Fusion: Meta-Analysis and Review of the Literature. Neurospine 2020, 17, 473. [Google Scholar] [CrossRef]
- Jain, S.; Eltorai, A.E.M.; Ruttiman, R.; Daniels, A.H. Advances in Spinal Interbody Cages. Orthop. Surg. 2016, 8, 278–284. [Google Scholar] [CrossRef]
- Tan, J.-H.; Cheong, C.K.; Hey, H.W.D. Titanium (Ti) Cages May Be Superior to Polyetheretherketone (PEEK) Cages in Lumbar Interbody Fusion: A Systematic Review and Meta-Analysis of Clinical and Radiological Outcomes of Spinal Interbody Fusions Using Ti versus PEEK Cages. Eur. Spine J. 2021, 30, 1285–1295. [Google Scholar] [CrossRef]
- Bao, Q.B.; McCullen, G.M.; Higham, P.A.; Dumbleton, J.H.; Yuan, H.A. The Artificial Disc: Theory, Design and Materials. Biomaterials 1996, 17, 1157–1167. [Google Scholar] [CrossRef]
- Othman, Y.A.; Verma, R.; Qureshi, S.A. Artificial Disc Replacement in Spine Surgery. Ann. Transl. Med. 2019, 7, S170. [Google Scholar] [CrossRef]
- Lemaire, J.P.; Carrier, H.; Ali, E.H.S.; Skalli, W.; Lavaste, F. Clinical and Radiological Outcomes with the CHARITÉTM Artificial Disc: A 10-Year Minimum Follow-Up. Clin. Spine Surg. 2005, 18, 353–359. [Google Scholar]
- Allen, M. Pacemakers and Implantable Cardioverter Defibrillators. Anaesthesia 2006, 61, 883–890. [Google Scholar] [CrossRef]
- Merritt, K.; Rodrigo, J.J. Immune Response to Synthetic Materials. Clin. Orthop. Relat. Res. 1996, 326, 71–79. [Google Scholar] [CrossRef]
- Hirshorn, M.S.; Holley, L.K.; Money, D.K.; Spector, M.; Young, F.A.; Hales, J.R. Histological Evaluation of Porous Titanium Cardiac Pacemaker Electrode Tips. J. Biomed. Mater. Res. 1984, 18, 47–60. [Google Scholar] [CrossRef] [PubMed]
- Norlin, A.; Pan, J.; Leygraf, C. Investigation of Pt, Ti, TiN, and Nano-Porous Carbon Electrodes for Implantable Cardioverter-Defibrillator Applications. Electrochim. Acta 2004, 49, 4011–4020. [Google Scholar] [CrossRef]
- Ahadi, F.; Azadi, M.; Biglari, M.; Bodaghi, M.; Khaleghian, A. Evaluation of Coronary Stents: A Review of Types, Materials, Processing Techniques, Design, and Problems. Heliyon 2023, 9, e13575. [Google Scholar] [CrossRef] [PubMed]
- Hanawa, T. Materials for Metallic Stents. J. Artif. Organs 2009, 12, 73–79. [Google Scholar] [CrossRef]
- Beshchasna, N.; Saqib, M.; Kraskiewicz, H.; Wasyluk, Ł.; Kuzmin, O.; Duta, O.C.; Ficai, D.; Ghizdavet, Z.; Marin, A.; Ficai, A.; et al. Recent Advances in Manufacturing Innovative Stents. Pharmaceutics 2020, 12, 349. [Google Scholar] [CrossRef] [PubMed]
- Beshchasna, N.; Ho, A.Y.K.; Saqib, M.; Kraśkiewicz, H.; Wasyluk, Ł.; Kuzmin, O.; Duta, O.C.; Ficai, D.; Trusca, R.D.; Ficai, A.; et al. Surface Evaluation of Titanium Oxynitride Coatings Used for Developing Layered Cardiovascular Stents. Mater. Sci. Eng. C Mater. Biol. Appl. 2019, 99, 405–416. [Google Scholar] [CrossRef] [PubMed]
- Bhuvaneshwar, G.S.; Muraleedharan, C.V.; Ramani, A.V.; Valiathan, M.S. Evaluation of Materials for Artificial Heart Valves. Bull. Mater. Sci. 1991, 14, 1363–1374. [Google Scholar] [CrossRef]
- Olszyna, A.; Smolik, J. Nanocrystalline Diamond-like Carbon Coatings Produced on the Si3N4–TiC Composites Intended for the Edges of Cutting Tools. Thin Solid Films 2004, 459, 224–227. [Google Scholar] [CrossRef]
- Dion, I.; Roques, X.; Baquey, C.; Baudet, E.; Basse Cathalinat, B.; More, N. Hemocompatibility of Diamond-like Carbon Coating. Biomed. Mater. Eng. 1993, 3, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Liu, X.; Mao, Y.; Huang, N.; Chen, Y.; Zheng, Z.; Zhou, Z.; Chen, A.; Jiang, Z. Artificial Heart Valves:: Improved Hemocompatibility by Titanium Oxide Coatings Prepared by Ion Beam Assisted Deposition. Surf. Coat. Technol. 1998, 103–104, 146–150. [Google Scholar] [CrossRef]
- Grenadyorov, A.S.; Zhulkov, M.O.; Solovyev, A.A.; Oskomov, K.V.; Semenov, V.A.; Chernyavskiy, A.M.; Sirota, D.A.; Karmadonova, N.A.; Malashchenko, V.V.; Litvinova, L.S.; et al. Surface Characterization and Biological Assessment of Corrosion-Resistant AC: H: SiOx PACVD Coating for Ti-6Al-4V Alloy. Mater. Sci. Eng. C. 2021, 123, 112002. [Google Scholar]
- Jiang, J.Y.; Xu, J.L.; Liu, Z.H.; Deng, L.; Sun, B.; Liu, S.D.; Wang, L.; Liu, H.Y. Preparation, Corrosion Resistance and Hemocompatibility of the Superhydrophobic TiO2 Coatings on Biomedical Ti-6Al-4V Alloys. Appl. Surf. Sci. 2015, 347, 591–595. [Google Scholar] [CrossRef]
- Asirvatham, A.; Devadoss, D.; Kujur, A.; Selvam, A.; Devi, J.N.; Mary, S.J. Anti Corrosion Activity of CRF (Cardiac Risk Free) Drug for SS316L, Ni-Ti, and Ti-6Al-4V in Artificial Blood Plasma. Chem. Afr. 2023, 29, 1–3. [Google Scholar] [CrossRef]
- Mohanta, M.; Thirugnanam, A. Commercial Pure Titanium—A Potential Candidate for Cardiovascular Stent. Materwiss. Werksttech. 2022, 53, 1518–1543. [Google Scholar] [CrossRef]
- Mohanta, M.; Thirugnanam, A. Evolution of Commercially Pure Titanium/Heparin/Poly (Ethylene Glycol) Substrate with Improved Biocompatibility for Cardiovascular Device Applications. Mater. Technol. 2022, 37, 3100–3109. [Google Scholar] [CrossRef]
- Bahl, S.; Aleti, B.T.; Suwas, S.; Chatterjee, K. Surface Nanostructuring of Titanium Imparts Multifunctional Properties for Orthopedic and Cardiovascular Applications. Mater. Des. 2018, 144, 169–181. [Google Scholar] [CrossRef]
- Nagaraja, S.; Brown, R.; Saylor, D.; Undisz, A. Oxide Layer Formation, Corrosion, and Biocompatibility of Nitinol Cardiovascular Devices. Shape Mem. Superelasticity 2022, 8, 45–63. [Google Scholar] [CrossRef]
- Wang, Y.; Wei, X.; Li, Z.; Sun, X.; Liu, H.; Jing, X.; Gong, Z. Experimental Investigation on the Effects of Different Electrolytic Polishing Solutions on Nitinol Cardiovascular Stents. J. Mater. Eng. Perform. 2021, 30, 4318–4327. [Google Scholar] [CrossRef]
- Beyar, R.; Henry, M.; Shofti, R.; Grenedier, E.; Globerman, O.; Beyar, M. Self-Expandable Nitinol Stent for Cardiovascular Applications: Canine and Human Experience. Cathet. Cardiovasc. Diagn. 1994, 32, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Shemyatovsky, K.A.; Azimov, R.H.; Alekhin, A.I.; Kazantsev, A.A.; Alekhin, A.A. Computed Tomography Options in the Evaluation of Hernia Repair Outcomes Using “Titanium Silk” Mesh Implants. J. Tissue Eng. Regen. Med. 2020, 14, 684–689. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y. Orbital Defect Repair and Secondary Reconstruction of Enophthalmos with Mirror-Technique Fabricated Titanium Mesh. J. Oral Maxillofac. Surg. 2008, 66, 19–20. [Google Scholar] [CrossRef]
- Sun, J.; Shen, Y.; Weng, Y.Q.; Li, J.; Zhang, Z.Y. Maxillary Reconstruction after Total Maxillectomy with Vascularised Fibula Osteomyocutaneous Flap and Titanium Mesh. Int. J. Oral Maxillofac. Surg. 2009, 38, 502. [Google Scholar] [CrossRef]
- Janssen, L.M.; van Osch, G.J.V.M.; Li, J.P.; Kops, N.; de Groot, K.; Feenstra, L.; Hardillo, J.A.U. Laryngotracheal Reconstruction with Porous Titanium in Rabbits: Are Vascular Carriers and Mucosal Grafts Really Necessary? J. Tissue Eng. Regen. Med. 2010, 4, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Pluhator-Murton, M.M.; Fedorak, R.N.; Audette, R.J.; Marriage, B.J.; Yatscoff, R.W.; Gramlich, L.M. Trace Element Contamination of Total Parenteral Nutrition. 1. Contribution of Component Solutions. JPEN J. Parenter. Enteral Nutr. 1999, 23, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Dean, J.A. Lange’s Handbook of Chemistry; Translated by V. Glyanchenko Tl; McGraw-Hill: New York, NY, USA, 1979. [Google Scholar]
- Saxena, M.; Loza-Rosas, S.A.; Gaur, K.; Sharma, S.; Pérez Otero, S.C.; Tinoco, A.D. Exploring Titanium(IV) Chemical Proximity to Iron(III) to Elucidate a Function for Ti(IV) in the Human Body. Coord. Chem. Rev. 2018, 363, 109–125. [Google Scholar] [CrossRef]
- McGarry, S.; Morgan, S.J.; Grosskreuz, R.M.; Williams, A.E.; Smith, W.R. Serum Titanium Levels in Individuals Undergoing Intramedullary Femoral Nailing with a Titanium Implant. J. Trauma 2008, 64, 430–433. [Google Scholar] [CrossRef]
- Fragata, M.; Bellemare, F. Dielectric Constant Dependence of Biological Oxidation-Reduction. 1. A Model of Polarity-Dependent Ferrocytochrome c Oxidation. Biophys. Chem. 1982, 15, 111–119. [Google Scholar] [CrossRef]
- Sundgren, J.-E.; Bodö, P.; Lundström, I. Auger Electron Spectroscopic Studies of the Interface between Human Tissue and Implants of Titanium and Stainless Steel. J. Colloid Interface Sci. 1986, 110, 9–20. [Google Scholar] [CrossRef]
- Albrektsson, T.; Brånemark, P.-I.; Hansson, H.-A.; Kasemo, B.; Larsson, K.; Lundström, I.; McQueen, D.H.; Skalak, R. The Interface Zone of Inorganic ImplantsIn Vivo: Titanium Implants in Bone. Ann. Biomed. Eng. 1983, 11, 1–27. [Google Scholar] [CrossRef]
- Kang, Y.; Li, X.; Tu, Y.; Wang, Q.; Ågren, H. On the Mechanism of Protein Adsorption onto Hydroxylated and Nonhydroxylated TiO2 Surfaces. J. Phys. Chem. C 2010, 114, 14496–14502. [Google Scholar] [CrossRef]
- Sousa, S.R.; Moradas-Ferreira, P.; Saramago, B.; Melo, L.V.; Barbosa, M.A. Human Serum Albumin Adsorption on TiO2 from Single Protein Solutions and from Plasma. Langmuir 2004, 20, 9745–9754. [Google Scholar] [CrossRef] [PubMed]
- Strehle, M.A.; Rösch, P.; Petry, R.; Hauck, A.; Thull, R.; Kiefer, W.; Popp, J. A Raman Spectroscopic Study of the Adsorption of Fibronectin and Fibrinogen on Titanium Dioxide Nanoparticles. Phys. Chem. Chem. Phys. 2004, 6, 5232–5236. [Google Scholar] [CrossRef]
- Tamura, R.N.; Oda, D.; Quaranta, V.; Plopper, G.; Lambert, R.; Glaser, S.; Jones, J.C. Coating of Titanium Alloy with Soluble Laminin-5 Promotes Cell Attachment and Hemidesmosome Assembly in Gingival Epithelial Cells: Potential Application to Dental Implants. J. Periodontal Res. 1997, 32, 287–294. [Google Scholar] [CrossRef]
- Ellingsen, J.E. A Study on the Mechanism of Protein Adsorption to TiO2. Biomaterials 1991, 12, 593–596. [Google Scholar] [CrossRef]
- Kulkarni, M.; Mazare, A.; Park, J.; Gongadze, E.; Killian, M.S.; Kralj, S.; von der Mark, K.; Iglič, A.; Schmuki, P. Protein Interactions with Layers of TiO2 Nanotube and Nanopore Arrays: Morphology and Surface Charge Influence. Acta Biomater. 2016, 45, 357–366. [Google Scholar] [CrossRef]
- Topoglidis, E.; Cass, A.E.; Gilardi, G.; Sadeghi, S.; Beaumont, N.; Durrant, J.R. Protein Adsorption on Nanocrystalline TiO2 Films: An Immobilization Strategy for Bioanalytical Devices. Anal. Chem. 1998, 70, 5111–5113. [Google Scholar] [CrossRef]
- Ranjan, S.; Dasgupta, N.; Chinnappan, S.; Ramalingam, C.; Kumar, A. Titanium Dioxide Nanoparticle–Protein Interaction Explained by Docking Approach. Int. J. Nanomed. 2018, 13, 47–50. [Google Scholar] [CrossRef]
- Li, N.; Xu, Z.; Zheng, S.; Dai, H.; Wang, L.; Tian, Y.; Dong, Z.; Jiang, L. Superamphiphilic TiO2 Composite Surface for Protein Antifouling. Adv. Mater. 2021, 33, e2003559. [Google Scholar] [CrossRef]
- Chen, Y.; Liu, Q.; Yu, H.; Guo, Y.; Cheng, Y.; Qian, H.; Xie, Y.; Yao, W. Protein Corona Formed on the TiO2 Nanoparticles Promotes the Hydrolysis of Collagen in Simulated Gastrointestinal Fluids. Food Biosci. 2023, 53, 102786. [Google Scholar] [CrossRef]
- Wang, Y.-Q.; Zhang, H.-M.; Wang, R.-H. Investigation of the Interaction between Colloidal TiO2 and Bovine Hemoglobin Using Spectral Methods. Colloids Surf. B Biointerfaces 2008, 65, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Kong, L.; Barber, T.; Aldinger, J.; Bowman, L.; Leonard, S.; Zhao, J.; Ding, M. ROS Generation Is Involved in Titanium Dioxide Nanoparticle-Induced AP-1 Activation through P38 MAPK and ERK Pathways in JB6 Cells. Environ. Toxicol. 2022, 37, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Martinet, W.; Knaapen, M.W.; De Meyer, G.R.; Herman, A.G.; Kockx, M.M. Oxidative DNA Damage and Repair in Experimental Atherosclerosis Are Reversed by Dietary Lipid Lowering. Circ. Res. 2001, 88, 733–739. [Google Scholar] [CrossRef] [PubMed]
- Charles, S.; Jomini, S.; Fessard, V.; Bigorgne-Vizade, E.; Rousselle, C.; Michel, C. Assessment of the in Vitro Genotoxicity of TiO2 Nanoparticles in a Regulatory Context. Nanotoxicology 2018, 12, 357–374. [Google Scholar] [CrossRef] [PubMed]
- Shukla, R.K.; Sharma, V.; Pandey, A.K.; Singh, S.; Sultana, S.; Dhawan, A. ROS-Mediated Genotoxicity Induced by Titanium Dioxide Nanoparticles in Human Epidermal Cells. Toxicol. Vitr. 2011, 25, 231–241. [Google Scholar] [CrossRef]
- Tan, K.S.; Qian, L.; Rosado, R.; Flood, P.M.; Cooper, L.F. The Role of Titanium Surface Topography on J774A.1 Macrophage Inflammatory Cytokines and Nitric Oxide Production. Biomaterials 2006, 27, 5170–5177. [Google Scholar] [CrossRef]
- Nowzari, H.; Botero, J.E.; DeGiacomo, M.; Villacres, M.C.; Rich, S.K. Microbiology and Cytokine Levels around Healthy Dental Implants and Teeth. Clin. Implant Dent. Relat. Res. 2008, 10, 166–173. [Google Scholar] [CrossRef]
- Preti, G.; Martinasso, G.; Peirone, B.; Navone, R.; Manzella, C.; Muzio, G.; Russo, C.; Canuto, R.A.; Schierano, G. Cytokines and Growth Factors Involved in the Osseointegration of Oral Titanium Implants Positioned Using Piezoelectric Bone Surgery versus a Drill Technique: A Pilot Study in Minipigs. J. Periodontol. 2007, 78, 716–722. [Google Scholar] [CrossRef]
- Pitchai, M.; Ipe, D.; Tadakamadla, S.; Hamlet, S. Titanium Implant Surface Effects on Adherent Macrophage Phenotype: A Systematic Review. Materials 2022, 15, 7314. [Google Scholar] [CrossRef]
- Krause, A.; Cowles, E.A.; Gronowicz, G. Integrin-Mediated Signaling in Osteoblasts on Titanium Implant Materials. J. Biomed. Mater. Res. 2000, 52, 738–747. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.-J.; Choi, M.-U.; Kim, C.-W. Activation of Phospholipase D1 by Surface Roughness of Titanium in MG63 Osteoblast-like Cell. Biomaterials 2006, 27, 5502–5511. [Google Scholar] [CrossRef] [PubMed]
- Berthet, J.-P.; Gomez Caro, A.; Solovei, L.; Gilbert, M.; Bommart, S.; Gaudard, P.; Canaud, L.; Alric, P.; Marty-Ané, C.-H. Titanium Implant Failure after Chest Wall Osteosynthesis. Ann. Thorac. Surg. 2015, 99, 1945–1952. [Google Scholar] [CrossRef] [PubMed]
- Shemtov-Yona, K.; Rittel, D. An Overview of the Mechanical Integrity of Dental Implants. Biomed Res. Int. 2015, 2015, 547384. [Google Scholar] [CrossRef] [PubMed]
- Kronström, M.; Svenson, B.; Hellman, M.; Persson, G.R. Early Implant Failures in Patients Treated with Brånemark System Titanium Dental Implants: A Retrospective Study. Int. J. Oral Maxillofac. Implants 2001, 16, 201–207. [Google Scholar] [PubMed]
- Iijima, R.; Ikari, Y.; Amiya, E.; Tanimoto, S.; Nakazawa, G.; Kyono, H.; Hatori, M.; Miyazawa, A.; Nakayama, T.; Aoki, J.; et al. The Impact of Metallic Allergy on Stent Implantation: Metal Allergy and Recurrence of in-Stent Restenosis. Int. J. Cardiol. 2005, 104, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Sanderson, P.J. Infection in Orthopaedic Implants. J. Hosp. Infect. 1991, 18, 367–375. [Google Scholar] [CrossRef]
- Trampuz, A.; Widmer, A.F. Infections Associated with Orthopedic Implants. Curr. Opin. Infect. Dis. 2006, 19, 349–356. [Google Scholar] [CrossRef]
- Yuan, K.; Chen, H.-L. Obesity and Surgical Site Infections Risk in Orthopedics: A Meta-Analysis. Int. J. Surg. 2013, 11, 383–388. [Google Scholar] [CrossRef]
- de Boer, A.S.; Mintjes-de Groot, A.J.; Severijnen, A.J.; van den Berg, J.M.; van Pelt, W. Risk Assessment for Surgical-Site Infections in Orthopedic Patients. Infect. Control Hosp. Epidemiol. 1999, 20, 402–407. [Google Scholar] [CrossRef]
- Fisichella, L.; Fenga, D.; Rosa, M.A. Surgical Site Infection in Orthopaedic Surgery: Correlation between Age, Diabetes, Smoke and Surgical Risk. Folia Med. 2014, 56, 259–263. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Singletary, R.; Schmader, K.; Anderson, D.J.; Bolognesi, M.; Kaye, K.S. Surgical Site Infection in the Elderly Following Orthopaedic Surgery. J. Bone Jt. Surg. Am. 2006, 88, 1705–1712. [Google Scholar] [CrossRef] [PubMed]
- Johansen, J.B.; Jørgensen, O.D.; Møller, M.; Arnsbo, P.; Mortensen, P.T.; Nielsen, J.C. Infection after Pacemaker Implantation: Infection Rates and Risk Factors Associated with Infection in a Population-Based Cohort Study of 46299 Consecutive Patients. Eur. Heart J. 2011, 32, 991–998. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, M.; Monteiro, F.J.; Ferraz, M.P. Infection of Orthopedic Implants with Emphasis on Bacterial Adhesion Process and Techniques Used in Studying Bacterial-Material Interactions. Biomatter 2012, 2, 176–194. [Google Scholar] [CrossRef] [PubMed]
- Hadeed, M.M.; Evans, C.L.; Werner, B.C.; Novicoff, W.M.; Weiss, D.B. Does External Fixator Pin Site Distance from Definitive Implant Affect Infection Rate in Pilon Fractures? Injury 2019, 50, 503–507. [Google Scholar] [CrossRef] [PubMed]
- Dombrowsky, A.; Abyar, E.; McGwin, G.; Johnson, M. Is Definitive Plate Fixation Overlap with External Fixator Pin Sites a Risk Factor for Infection in Pilon Fractures? J. Orthop. Trauma 2021, 35, e7–e12. [Google Scholar] [CrossRef] [PubMed]
- Mosseri, M.; Miller, H.; Tamari, I.; Plich, M.; Hasin, Y.; Brizines, M.; Frimerman, A.; Jefary, J.; Guetta, V.; Solomon, M.; et al. The Titanium-NO Stent:Results of a Multicenter Registry. EuroIntervention 2006, 2, 192–196. [Google Scholar] [PubMed]
- Mazzaccaro, D.; Giannetta, M.; Fancoli, F.; Righini, P.; Nano, G. Endovascular Treatment of Extracranial Carotid Artery Stenosis Using a Dual-Layer Micromesh Stents: A Systematic Review. Expert Rev. Med. Devices 2021, 18, 545–552. [Google Scholar] [CrossRef]
- Tortamano, P.; Camargo, L.O.A.; Bello-Silva, M.S.; Kanashiro, L.H. Immediate Implant Placement and Restoration in the Esthetic Zone: A Prospective Study with 18 Months of Follow-Up. Int. J. Oral Maxillofac. Implants 2010, 25, 345–350. [Google Scholar]
- Sezai, A.; Akiyama, K.; Hata, M.; Niino, T.; Yoshitake, I.; Wakui, S.; Fujita, K.; Takasaka, A.; Kawachi, H.; Murakami, T.; et al. Total Arch Replacement and Open Stent Graft Implantation Using a Newly Developed Stent Graft: Report of a Case. Surg. Today 2011, 41, 396–398. [Google Scholar] [CrossRef]
- Valdés Chavarri, M.; Bethencourt, A.; Pinar, E.; Gomez, A.; Portales, J.F.; Pomar, F.; Calvo, I.; López-Minguez, J.R.; Valdesuso, R.; Moreu, J.; et al. Titanium-Nitride-OxIde-Coated Stents Multicenter Registry in DiaBEtic PatienTs: The TIBET Registry. Heart Vessels 2012, 27, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Sbordone, L.; Toti, P.; Menchini-Fabris, G.; Sbordone, C.; Guidetti, F. Implant Survival in Maxillary and Mandibular Osseous Onlay Grafts and Native Bone: A 3-Year Clinical and Computerized Tomographic Follow-Up. Int. J. Oral Maxillofac. Implants 2009, 24, 695–703. [Google Scholar] [PubMed]
- Ma, L.; Zhou, Y.; Zhu, Y.; Lin, Z.; Chen, L.; Zhang, Y.; Xia, H.; Mao, C. 3D Printed Personalized Titanium Plates Improve Clinical Outcome in Microwave Ablation of Bone Tumors around the Knee. Sci. Rep. 2017, 7, 7626. [Google Scholar] [CrossRef] [PubMed]
- Martola, M.; Lindqvist, C.; Hänninen, H.; Al-Sukhun, J. Fracture of Titanium Plates Used for Mandibular Reconstruction Following Ablative Tumor Surgery. J. Biomed. Mater. Res. B Appl. Biomater. 2007, 80, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Irish, J.C.; Gullane, P.J.; Gilbert, R.W.; Brown, D.H.; Birt, B.D.; Boyd, J.B. Primary Mandibular Reconstruction with the Titanium Hollow Screw Reconstruction Plate: Evaluation of 51 Cases. Plast. Reconstr. Surg. 1995, 96, 93–99. [Google Scholar] [CrossRef]
- Jain, N.S.; Hah, R.J. Pedicle Screw Fixation. In Handbook of Spine Technology; Springer International Publishing: Cham, Switzerland, 2021; pp. 541–560. ISBN 9783319444239. [Google Scholar]
- Allam, A.F.A.; Allam, M.F.A.; Koptan, W.; Abotakia, T.A.A. Pedicle Screw/Sublaminar Hook Fixation versus Pedicle Screw/Infraspinous Wire Fixation for Spondylolysis Repair: A Retrospective Comparative Study with MSCT Assessment. Egypt. Spine J. 2023, 41, 7. [Google Scholar] [CrossRef]
- Changoor, S.; Faloon, M.J.; Dunn, C.J.; Sahai, N.; Issa, K.; Sinha, K.; Hwang, K.S.; Emami, A. Does Percutaneous Lumbosacral Pedicle Screw Instrumentation Prevent Long-Term Adjacent Segment Disease after Lumbar Fusion? Asian Spine J. 2021, 15, 301–307. [Google Scholar] [CrossRef]
- Wedin, R.; Hansen, B.H.; Laitinen, M.; Trovik, C.; Zaikova, O.; Bergh, P.; Kalén, A.; Schwarz-Lausten, G.; Vult von Steyern, F.; Walloe, A.; et al. Complications and Survival after Surgical Treatment of 214 Metastatic Lesions of the Humerus. J. Shoulder Elbow Surg. 2012, 21, 1049–1055. [Google Scholar] [CrossRef]
- Miwa, S.; Shirai, T.; Yamamoto, N.; Hayashi, K.; Takeuchi, A.; Tada, K.; Kajino, Y.; Higuchi, T.; Abe, K.; Aiba, H.; et al. Risk Factors for Surgical Site Infection after Malignant Bone Tumor Resection and Reconstruction. BMC Cancer 2019, 19, 33. [Google Scholar] [CrossRef]
- Machecourt, J.; Danchin, N.; Lablanche, J.M.; Fauvel, J.M.; Bonnet, J.L.; Marliere, S.; Foote, A.; Quesada, J.L.; Eltchaninoff, H.; Vanzetto, G.; et al. Risk Factors for Stent Thrombosis after Implantation of Sirolimus-Eluting Stents in Diabetic and Nondiabetic Patients: The EVASTENT Matched-Cohort Registry. J. Am. Coll. Cardiol. 2007, 50, 501–508. [Google Scholar] [CrossRef]
- Hawn, M.T.; Graham, L.A.; Richman, J.S.; Itani, K.M.F.; Henderson, W.G.; Maddox, T.M. Risk of Major Adverse Cardiac Events Following Noncardiac Surgery in Patients with Coronary Stents. Surv. Anesthesiol. 2014, 58, 291. [Google Scholar] [CrossRef]
- Costanzo, R.; Ferini, G.; Brunasso, L.; Bonosi, L.; Porzio, M.; Benigno, U.E.; Musso, S.; Gerardi, R.M.; Giammalva, G.R.; Paolini, F.; et al. The Role of 3D-Printed Custom-Made Vertebral Body Implants in the Treatment of Spinal Tumors: A Systematic Review. Life 2022, 12, 489. [Google Scholar] [CrossRef] [PubMed]
- Bridwell, K.H.; Baldus, C.; Berven, S.; Edwards, C., 2nd; Glassman, S.; Hamill, C.; Horton, W.; Lenke, L.G.; Ondra, S.; Schwab, F.; et al. Changes in Radiographic and Clinical Outcomes with Primary Treatment Adult Spinal Deformity Surgeries from Two Years to Three- to Five-Years Follow-Up. Spine 2010, 35, 1849–1854. [Google Scholar] [CrossRef] [PubMed]
- David, T. Long-Term Results of One-Level Lumbar Arthroplasty: Minimum 10-Year Follow-up of the CHARITE Artificial Disc in 106 Patients. Spine 2007, 32, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Cook, S.; Asher, M.; Lai, S.-M.; Shobe, J. Reoperation after Primary Posterior Instrumentation and Fusion for Idiopathic Scoliosis. Spine 2000, 25, 463–468. [Google Scholar] [CrossRef] [PubMed]
- Bago, J.; Ramirez, M.; Pellise, F.; Villanueva, C. Survivorship Analysis of Cotrel-Dubousset Instrumentation in Idiopathic Scoliosis. Eur. Spine J. 2003, 12, 435–439. [Google Scholar] [CrossRef] [PubMed]
- Richards, B.S. Delayed Infections Following Posterior Spinal Instrumentation for the Treatment of Idiopathic Scoliosis. J. Bone Jt. Surg. Am. 1995, 77, 524–529. [Google Scholar] [CrossRef] [PubMed]
- Pompa, G.; Saccucci, M.; Di Carlo, G.; Brauner, E.; Valentini, V.; Di Carlo, S.; Gentile, T.; Guarino, G.; Polimeni, A. Survival of Dental Implants in Patients with Oral Cancer Treated by Surgery and Radiotherapy: A Retrospective Study. BMC Oral Health 2015, 15, 5. [Google Scholar] [CrossRef]
- Cheung, L.K.; Leung, A.C.F. Dental Implants in Reconstructed Jaws: Implant Longevity and Peri-Implant Tissue Outcomes. J. Oral Maxillofac. Surg. 2003, 61, 1263–1274. [Google Scholar] [CrossRef]
- Alfaro, M.F.; Rossman, P.K.; Viera Marques, I.D.S.; Dube, A.; Takoudis, C.; Shokuhfar, T.; Mathew, M.T.; Sukotjo, C. Interface Damage in Titanium Dental Implant Due to Tribocorrosion: The Role of Mastication Frequencies. J. Bio-Tribo-Corros. 2019, 5, 1–2. [Google Scholar] [CrossRef]
- Gao, S.-S.; Zhang, Y.-R.; Zhu, Z.-L.; Yu, H.-Y. Micromotions and Combined Damages at the Dental Implant/Bone Interface. Int. J. Oral Sci. 2012, 4, 182–188. [Google Scholar] [CrossRef] [PubMed]
- van der Bilt, A.; Engelen, L.; Pereira, L.J.; van der Glas, H.W.; Abbink, J.H. Oral Physiology and Mastication. Physiol. Behav. 2006, 89, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Pileicikiene, G.; Surna, A. The Human Masticatory System from a Biomechanical Perspective: A Review. Stomatologija 2004, 6, 81–84. [Google Scholar]
- Takamiya, A.S.; Goiato, M.C.; Gennari Filho, H. Effect of Smoking on the Survival of Dental Implants. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czech. Repub. 2014, 158, 650–653. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Bae, J.-H.; Kim, Y.-K. Implant Prosthetic Complications, Fractures of the Implant Fixtures—Retrospective Clinical Study. Clin. Oral Implant. Res. 2019, 30, 342. [Google Scholar] [CrossRef]
- Sedghi, L.; DiMassa, V.; Harrington, A.; Lynch, S.V.; Kapila, Y.L. The Oral Microbiome: Role of Key Organisms and Complex Networks in Oral Health and Disease. Periodontology 2000 2021, 87, 107–131. [Google Scholar] [CrossRef] [PubMed]
- Lakshmi Bolla, V.; Munnangi, S.R.; Chowdary, U.K.; Koppulu, P.; Swapna, L.A. Correlation between the PH of Saliva, Plaque and Buffering Capacity of Saliva. Int. J. Appl. Dent. Sci. 2017, 53, 48–50. [Google Scholar]
- Wirtz, D.C.; Gravius, S.; Ascherl, R.; Thorweihe, M.; Forst, R.; Noeth, U.; Maus, U.M.; Wimmer, M.D.; Zeiler, G.; Deml, M.C. Uncemented Femoral Revision Arthroplasty Using a Modular Tapered, Fluted Titanium Stem: 5- to 16-Year Results of 163 Cases. Acta Orthop. 2014, 85, 562–569. [Google Scholar] [CrossRef]
- Rodriguez, J.A.; Deshmukh, A.J.; Robinson, J.; Cornell, C.N.; Rasquinha, V.J.; Ranawat, A.S.; Ranawat, C.S. Reproducible Fixation with a Tapered, Fluted, Modular, Titanium Stem in Revision Hip Arthroplasty at 8–15 Years Follow-Up. J. Arthroplast. 2014, 29, 214–218. [Google Scholar] [CrossRef]
- Aoki, Y.; Tome, Y.; Oshiro, H.; Mizuta, K.; Katsuki, R.; Hoffman, R.M.; Nishida, K. Long-Lasting Limb Salvage after Malignant Femoral-Bone Tumor Resection Reconstructed with a Thin-Mantle Titanium Stem Fixated with Cement. Anticancer Res. 2023, 43, 3507–3511. [Google Scholar] [CrossRef]
- Zampieri, A.; Lukas, S.; Ibrahim, M.; Talbi, A.; Prodhomme, G.; Chantelot, C. Cementless, Modular, Titanium Stem in Vancouver B2 and B3 Periprosthetic Femoral Fractures. Eur. J. Orthop. Surg. Traumatol. 2023, 33, 1133–1139. [Google Scholar] [CrossRef] [PubMed]
- Eingartner, C.; Ihm, A.; Maurer, F.; Volkmann, R.; Weise, K.; Weller, S. Good long term results with a cemented straight femoral shaft prosthesis made of titanium. Unfallchirurg 2002, 105, 804–810. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, M.; Tone, S.; Naito, Y.; Wakabayashi, H.; Sudo, A. Minimum Ten-Year Results in Revision Total Hip Arthroplasty Using Titanium Fully Porous Long Stem. Int. Orthop. 2021, 45, 1727–1733. [Google Scholar] [CrossRef] [PubMed]
- Takaoka, Y.; Goto, K.; Kuroda, Y.; Kawai, T.; Matsuda, S. The Long-Term Results of Total Hip Arthroplasty with a Cemented β-Titanium Stem. J. Arthroplast. 2020, 35, 2167–2172. [Google Scholar] [CrossRef] [PubMed]
- Carlson, S.W.; Goetz, D.D.; Liu, S.S.; Greiner, J.J.; Callaghan, J.J. Minimum 10-Year Follow-up of Cementless Total Hip Arthroplasty Using a Contemporary Triple-Tapered Titanium Stem. J. Arthroplasty 2016, 31, 2231–2236. [Google Scholar] [CrossRef]
- Akiyama, H.; Kawanabe, K.; Yamamoto, K.; So, K.; Kuroda, Y.; Nakamura, T. Clinical Outcomes of Cemented Double-Tapered Titanium Femoral Stems: A Minimum 5-Year Follow-Up. J. Orthop. Sci. 2011, 16, 689–697. [Google Scholar] [CrossRef]
- Danesh-Clough, T.; Bourne, R.B.; Rorabeck, C.H.; McCalden, R. The Mid-Term Results of a Dual Offset Uncemented Stem for Total Hip Arthroplasty. J. Arthroplast. 2007, 22, 195–203. [Google Scholar] [CrossRef]
- Goetz, D.D.; Reddy, A.; Callaghan, J.J.; Hennessy, D.W.; Bedard, N.A.; Liu, S.S. Four- to Six-Year Follow-up of Primary THA Using Contemporary Titanium Tapered Stems. Orthopedics 2013, 36, e1521–e1526. [Google Scholar] [CrossRef]
- Han, C.-D.; Shin, K.-Y.; Lee, H.-H.; Park, K.-K.; Yang, I.-H.; Lee, W.-S. The Results of Long-Term Follow-up of Total Hip Arthroplasty Using Hydroxyapatite-Coated Cups. Hip Pelvis 2015, 27, 209–215. [Google Scholar] [CrossRef]
- Reikerås, O. Total Hip Arthroplasty with a Fully Hydroxyapatite Coated Stem: A Cohort Study during Twenty Three to Twenty Eight Years. J. Arthroplast. 2017, 32, 1543–1546. [Google Scholar] [CrossRef]
- Aldinger, P.R.; Jung, A.W.; Pritsch, M.; Breusch, S.; Thomsen, M.; Ewerbeck, V.; Parsch, D. Uncemented Grit-Blasted Straight Tapered Titanium Stems in Patients Younger than Fifty-Five Years of Age. Fifteen to Twenty-Year Results. J. Bone Jt. Surg. Am. 2009, 91, 1432–1439. [Google Scholar] [CrossRef] [PubMed]
- Aldinger, P.R.; Thomsen, M.; Mau, H.; Ewerbeck, V.; Breusch, S.J. Cementless Spotorno Tapered Titanium Stems: Excellent 10-15-Year Survival in 141 Young Patients. Acta Orthop. Scand. 2003, 74, 253–258. [Google Scholar] [CrossRef]
- Streit, M.R.; Innmann, M.M.; Merle, C.; Bruckner, T.; Aldinger, P.R.; Gotterbarm, T. Long-Term (20- to 25-Year) Results of an Uncemented Tapered Titanium Femoral Component and Factors Affecting Survivorship. Clin. Orthop. Relat. Res. 2013, 471, 3262–3269. [Google Scholar] [CrossRef] [PubMed]
- Philippot, R.; Farizon, F.; Camilleri, J.-P.; Boyer, B.; Derhi, G.; Bonnan, J.; Fessy, M.-H.; Lecuire, F. Survival of Cementless Dual Mobility Socket with a Mean 17 Years Follow-Up. Rev. Chir. Orthop. Reparatrice Appar. Mot. 2008, 94, e23–e27. [Google Scholar] [CrossRef]
- Delaunay, C.; Hamadouche, M.; Girard, J.; Duhamel, A.; SoFCOT Group. What are the Causes for Failures of Primary Hip Arthroplasties in France? Clin. Orthop. Relat. Res. 2013, 471, 3863–3869. [Google Scholar] [CrossRef] [PubMed]
- Simka, W.; Iwaniak, A.; Nawrat, G.; Maciej, A.; Michalska, J.; Radwański, K.; Gazdowicz, J. Modification of Titanium Oxide Layer by Calcium and Phosphorus. Electrochim. Acta 2009, 54, 6983–6988. [Google Scholar] [CrossRef]
- Zhu, Y.; Wang, W.; Jia, X.; Akasaka, T.; Liao, S.; Watari, F. Deposition of TiC Film on Titanium for Abrasion Resistant Implant Material by Ion-Enhanced Triode Plasma CVD. Appl. Surf. Sci. 2012, 262, 156–158. [Google Scholar] [CrossRef]
- Jergesen, H.E.; Karlen, J.W. Clinical Outcome in Total Hip Arthroplasty Using a Cemented Titanium Femoral Prosthesis. J. Arthroplasty 2002, 17, 592–599. [Google Scholar] [CrossRef]
- Najjar, D.; Bigerelle, M.; Migaud, H.; Iost, A. Identification of Scratch Mechanisms on a Retrieved Metallic Femoral Head. Wear 2005, 258, 240–250. [Google Scholar] [CrossRef]
- Łapaj, Ł.; Wendland, J.; Markuszewski, J.; Mróz, A.; Wiśniewski, T. Retrieval Analysis of Titanium Nitride (TiN) Coated Prosthetic Femoral Heads Articulating with Polyethylene. J. Mech. Behav. Biomed. Mater. 2015, 55, 127–139. [Google Scholar] [CrossRef]
- Marin, E.; Offoiach, R.; Regis, M.; Fusi, S.; Lanzutti, A.; Fedrizzi, L. Diffusive Thermal Treatments Combined with PVD Coatings for Tribological Protection of Titanium Alloys. Mater. Des. 2016, 89, 314–322. [Google Scholar] [CrossRef]
- Hauert, R. A Review of Modified DLC Coatings for Biological Applications. Diam. Relat. Mater. 2003, 12, 583–589. [Google Scholar] [CrossRef]
- Malisz, K.; Świeczko-Żurek, B.; Sionkowska, A. Preparation and Characterization of Diamond-like Carbon Coatings for Biomedical Applications-A Review. Materials 2023, 16, 3420. [Google Scholar] [CrossRef] [PubMed]
- Hamada, K.; Kon, M.; Hanawa, T.; Yokoyama, K.; Miyamoto, Y.; Asaoka, K. Hydrothermal Modification of Titanium Surface in Calcium Solutions. Biomaterials 2002, 23, 2265–2272. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Jiang, T.; Zhou, Y.; Zhang, Z.; Wang, Z.; Tong, H.; Shen, X.; Wang, Y. Evaluation of the Attachment, Proliferation, and Differentiation of Osteoblast on a Calcium Carbonate Coating on Titanium Surface. Mater. Sci. Eng. C Mater. Biol. Appl. 2011, 31, 1055–1061. [Google Scholar] [CrossRef]
- Canillas, M.; Pena, P.; de Aza, A.H.; Rodríguez, M.A. Calcium Phosphates for Biomedical Applications. Bol. Soc. Esp. Ceram. Vidr. 2017, 56, 91–112. [Google Scholar] [CrossRef]
- Montazerian, M.; Hosseinzadeh, F.; Migneco, C.; Fook, M.V.L.; Baino, F. Bioceramic Coatings on Metallic Implants: An Overview. Ceram. Int. 2022, 48, 8987–9005. [Google Scholar] [CrossRef]
- DileepKumar, V.G.; Sridhar, M.S.; Aramwit, P.; Krut’ko, V.K.; Musskaya, O.N.; Glazov, I.E.; Reddy, N. A Review on the Synthesis and Properties of Hydroxyapatite for Biomedical Applications. J. Biomater. Sci. Polym. Ed. 2022, 33, 229–261. [Google Scholar] [CrossRef]
- Zhecheva, A.; Sha, W.; Malinov, S.; Long, A. Enhancing the Microstructure and Properties of Titanium Alloys through Nitriding and Other Surface Engineering Methods. Surf. Coat. Technol. 2005, 200, 2192–2207. [Google Scholar] [CrossRef]
- Schaaf, P.; Kaspar, J.; Höche, D. Laser Gas–Assisted Nitriding of Ti Alloys. In Comprehensive Materials Processing; Elsevier: Amsterdam, The Netherlands, 2014; Volume 9, pp. 261–278. ISBN 9780080965338. [Google Scholar]
- Kamat, A.M.; Copley, S.M.; Segall, A.E.; Todd, J.A. Laser-Sustained Plasma (LSP) Nitriding of Titanium: A Review. Coatings 2019, 9, 283. [Google Scholar] [CrossRef]
- Lanzutti, A.; Raffaelli, A.; Magnan, M.; Fedrizzi, L.; Regis, M.; Marin, E. Microstructural and Mechanical Study of an Induction Nitrided Ti Gr. 5 Hip Prosthesis Component. Surf. Coat. Technol. 2019, 377, 124895. [Google Scholar] [CrossRef]
- Zhecheva, A.; Malinov, S.; Sha, W. Titanium Alloys after Surface Gas Nitriding. Surf. Coat. Technol. 2006, 201, 2467–2474. [Google Scholar] [CrossRef]
- Morita, T.; Takahashi, H.; Shimizu, M.; Kawasaki, K. Factors Controlling the Fatigue Strength of Nitrided Titanium. Fatigue Fract. Eng. Mater. Struct. 1997, 20, 85–92. [Google Scholar] [CrossRef]
- Oliveira, W.F.; Arruda, I.R.S.; Silva, G.M.M.; Machado, G.; Coelho, L.C.B.B.; Correia, M.T.S. Functionalization of Titanium Dioxide Nanotubes with Biomolecules for Biomedical Applications. Mater. Sci. Eng. C Mater. Biol. Appl. 2017, 81, 597–606. [Google Scholar] [CrossRef] [PubMed]
- Schliephake, H.; Scharnweber, D. Chemical and Biological Functionalization of Titanium for Dental Implants. J. Mater. Chem. 2008, 18, 2404. [Google Scholar] [CrossRef]
- Kashiwagi, K.; Tsuji, T.; Shiba, K. Directional BMP-2 for Functionalization of Titanium Surfaces. Biomaterials 2009, 30, 1166–1175. [Google Scholar] [CrossRef] [PubMed]
- Royhman, D.; Patel, M.; Runa, M.J.; Jacobs, J.J.; Hallab, N.J.; Wimmer, M.A.; Mathew, M.T. Fretting-Corrosion in Hip Implant Modular Junctions: New Experimental Set-up and Initial Outcome. Tribol. Int. 2015, 91, 235–245. [Google Scholar] [CrossRef]
- Hoeppner, D.W.; Chandrasekaran, V. Fretting in Orthopaedic Implants: A Review. Wear 1994, 173, 189–197. [Google Scholar] [CrossRef]
- Ouellette, E.S.; Mali, S.A.; Kim, J.; Grostefon, J.; Gilbert, J.L. Design, Material, and Seating Load Effects on in Vitro Fretting Corrosion Performance of Modular Head-Neck Tapers. J. Arthroplasty 2019, 34, 991–1002. [Google Scholar] [CrossRef]
- Guan, J.; Jiang, X.; Xiang, Q.; Yang, F.; Liu, J. Corrosion and Tribocorrosion Behavior of Titanium Surfaces Designed by Electromagnetic Induction Nitriding for Biomedical Applications. Surf. Coat. Technol. 2021, 409, 126844. [Google Scholar] [CrossRef]
- Szymczyk, P.; Junka, A.; Ziółkowski, G.; Smutnicka, D.; Bartoszewicz, M.; Chlebus, E. The Ability of S. Aureus to Form Biofilm on the Ti-6Al-7Nb Scaffolds Produced by Selective Laser Melting and Subjected to the Different Types of Surface Modifications. Acta Bioeng. Biomech. 2013, 15, 69–76. [Google Scholar] [PubMed]
- Baume, A.S.; Boughton, P.C.; Coleman, N.V.; Ruys, A.J. Sterilization of Tissue Scaffolds. In Characterisation and Design of Tissue Scaffolds; Elsevier: Amsterdam, The Netherlands, 2016; pp. 225–244. ISBN 9781782420873. [Google Scholar]
- Tan, X.P.; Tan, Y.J.; Chow, C.S.L.; Tor, S.B.; Yeong, W.Y. Metallic Powder-Bed Based 3D Printing of Cellular Scaffolds for Orthopaedic Implants: A State-of-the-Art Review on Manufacturing, Topological Design, Mechanical Properties and Biocompatibility. Mater. Sci. Eng. C 2017, 76, 1328–1343. [Google Scholar] [CrossRef] [PubMed]
- Sidambe, A.T. Biocompatibility of advanced manufactured titanium implants—A review. Materials 2014, 7, 8168–8188. [Google Scholar] [CrossRef] [PubMed]
- Parithimarkalaignan, S.; Padmanabhan, T.V. Osseointegration: An update. J. Indian Prosthodont. Soc. 2013, 13, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Cui, C.; Hu, B.; Zhao, L.; Liu, S. Titanium alloy production technology, market prospects and industry development. Mater. Des. 2011, 2, 1684–1691. [Google Scholar] [CrossRef]
- Silva, D.; Arcos, C.; Montero, C.; Guerra, C.; Martínez, C.; Li, X.; Ringuedé, A.; Cassir, M.; Ogle, K.; Guzmán, D.; et al. A tribological and ion released research of Ti-materials for medical devices. Materials 2022, 15, 131. [Google Scholar] [CrossRef]
- Mohammed, M.T.; Khan, Z.A.; Siddiquee, A.N. Beta titanium alloys: The lowest elastic modulus for biomedical applications: A review. Int. J. Chem. Mol. Nucl. Mater. Metall. Eng. 2014, 8, 726–731. [Google Scholar]
- Senopati, G.; Rahman Rashid, R.A.; Kartika, I.; Palanisamy, S. Recent Development of Low-Cost β-Ti Alloys for Biomedical Applications: A Review. Metals 2023, 13, 194. [Google Scholar] [CrossRef]
- Manam, N.S.; Harun, W.S.W.; Shri, D.N.A.; Ghani, S.A.C.; Kurniawan, T.; Ismail, M.H.; Ibrahim, M.H.I. Study of corrosion in biocompatible metals for implants: A review. J. Alloys Compd. 2017, 701, 698–715. [Google Scholar] [CrossRef]
- Shastri, V.P. Non-degradable biocompatible polymers in medicine: Past, present and future. Curr. Pharm. Biotechnol. 2003, 4, 331–337. [Google Scholar] [CrossRef]
- Verma, S.; Sharma, N.; Kango, S.; Sharma, S. Developments of PEEK (Polyetheretherketone) as a biomedical material: A focused review. Eur. Polym. J. 2021, 147, 110295. [Google Scholar] [CrossRef]
- Pituru, S.M.; Greabu, M.; Totan, A.; Imre, M.; Pantea, M.; Spinu, T.; Tancu, A.M.C.; Popoviciu, N.O.; Stanescu, I.I.; Ionescu, E. A review on the biocompatibility of PMMA-based dental materials for interim prosthetic restorations with a glimpse into their modern manufacturing techniques. Materials 2020, 13, 2894. [Google Scholar] [CrossRef] [PubMed]
- Paxton, N.C.; Allenby, M.C.; Lewis, P.M.; Woodruff, M.A. Biomedical applications of polyethylene. Eur. Polym. J. 2019, 118, 412–428. [Google Scholar] [CrossRef]
- Delfi, M.; Ghomi, M.; Zarrabi, A.; Mohammadinejad, R.; Taraghdari, Z.B.; Ashrafizadeh, M.; Zare, E.N.; Agarwal, T.; Padil, V.V.; Mokhtari, B.; et al. Functionalization of polymers and nanomaterials for biomedical applications: Antimicrobial platforms and drug carriers. Prosthesis 2020, 2, 12. [Google Scholar] [CrossRef]
- Sun, W.; Liu, W.; Wu, Z.; Chen, H. Chemical surface modification of polymeric biomaterials for biomedical applications. Macromol. Rapid Commun. 2020, 41, 1900430. [Google Scholar] [CrossRef]
Figure 1.
Summary diagram of the contents of this review, with the numbers and titles of sections and sub-sections.
Figure 1.
Summary diagram of the contents of this review, with the numbers and titles of sections and sub-sections.

Figure 2.
Effects of (a) alpha and (b) beta stabilizers on the microstructure of titanium alloys. The dotted black lines represent the region of metastability of α-β alloys, the red dotted lines represent the expected microstructure at room temperature, (c) an example of a typical commercially pure α-titanium microstructure, and (d) an example of a typical annealed Ti-6Al-4V α-β alloy microstructure.
Figure 2.
Effects of (a) alpha and (b) beta stabilizers on the microstructure of titanium alloys. The dotted black lines represent the region of metastability of α-β alloys, the red dotted lines represent the expected microstructure at room temperature, (c) an example of a typical commercially pure α-titanium microstructure, and (d) an example of a typical annealed Ti-6Al-4V α-β alloy microstructure.


Figure 3.
Relationship between ultimate strength and elastic modulus for a selection of alloys commonly applied in the biomedical field, grouped by chemical composition.
Figure 3.
Relationship between ultimate strength and elastic modulus for a selection of alloys commonly applied in the biomedical field, grouped by chemical composition.

Figure 4.
Relationship between the ultimate tensile strength and the qualitative corrosion resistance of titanium alloys applied in the biomedical field. The colored areas indicate the kind of alloys.
Figure 4.
Relationship between the ultimate tensile strength and the qualitative corrosion resistance of titanium alloys applied in the biomedical field. The colored areas indicate the kind of alloys.

Figure 5.
Implant failures divided by category, going from 0% (in the center of the triangle) to 100% (at the outermost corners) of the failures.
Figure 5.
Implant failures divided by category, going from 0% (in the center of the triangle) to 100% (at the outermost corners) of the failures.

Figure 6.
Survival rate over time for different categories of titanium biomedical devices.

Figure 7.
Examples of (a) fretting damage after 5 years in vivo and (b) mechanical failure due to fretting corrosion after just 2 years in vivo for Ti-6Al-4V tapers in modular femoral stems.
Figure 7.
Examples of (a) fretting damage after 5 years in vivo and (b) mechanical failure due to fretting corrosion after just 2 years in vivo for Ti-6Al-4V tapers in modular femoral stems.


{kind=link}
{kind=link}
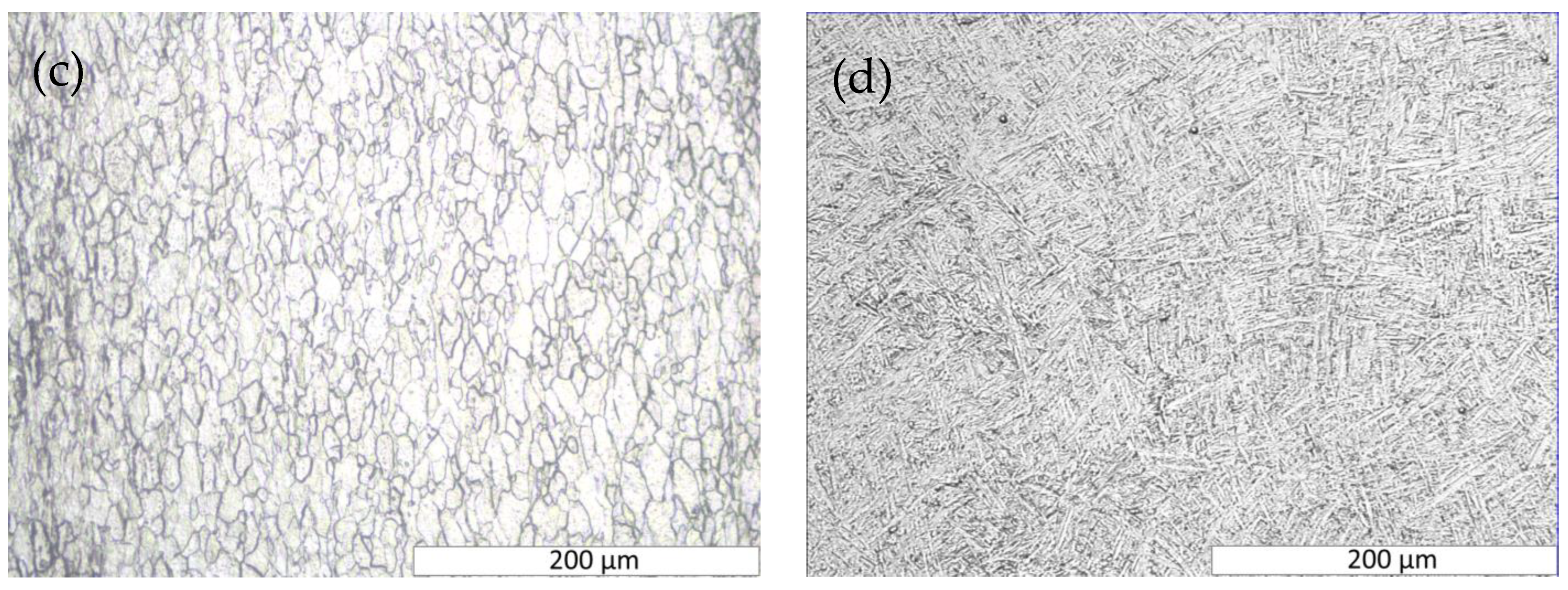{kind=link}
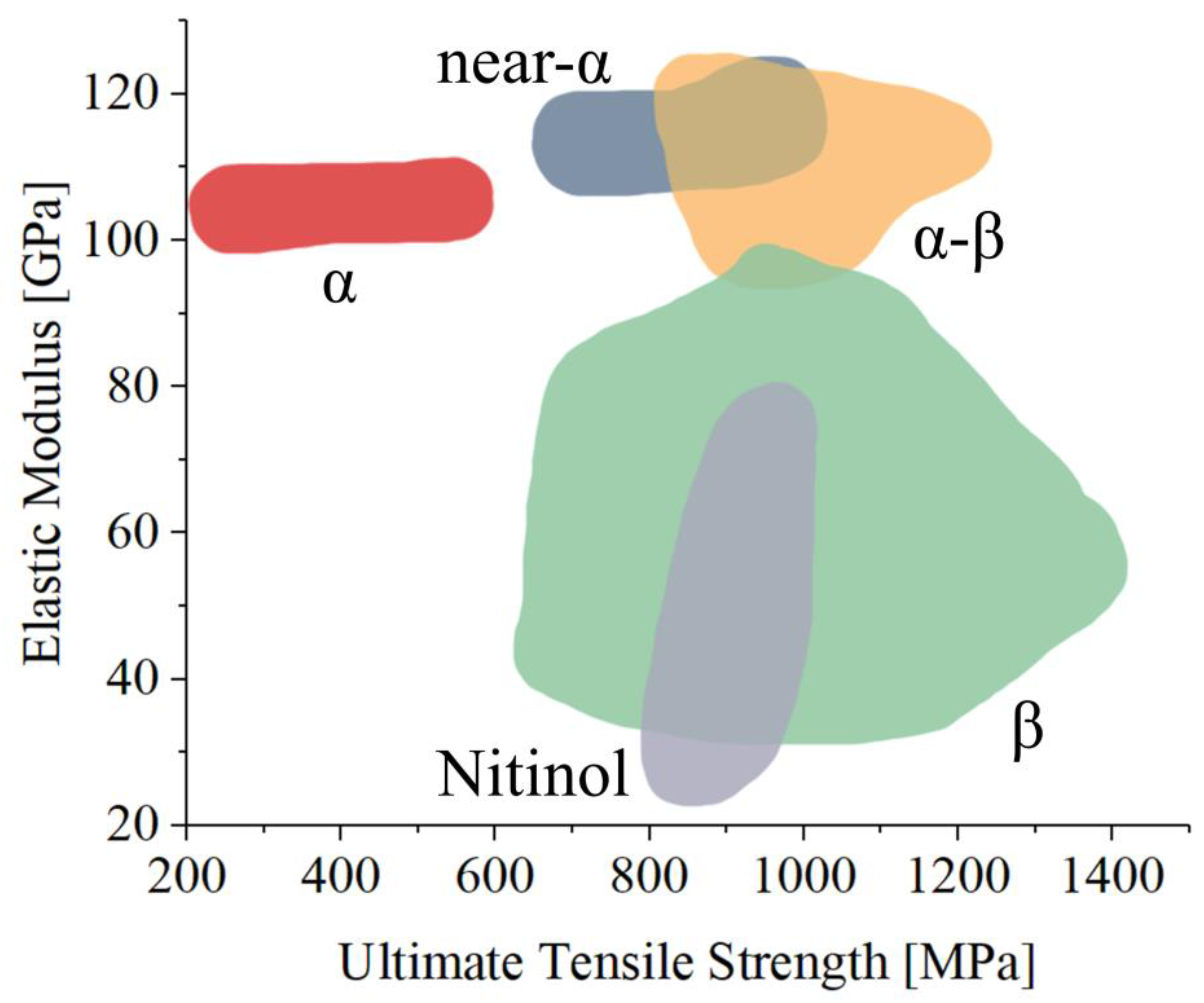{kind=link}
{kind=link}
{kind=link}
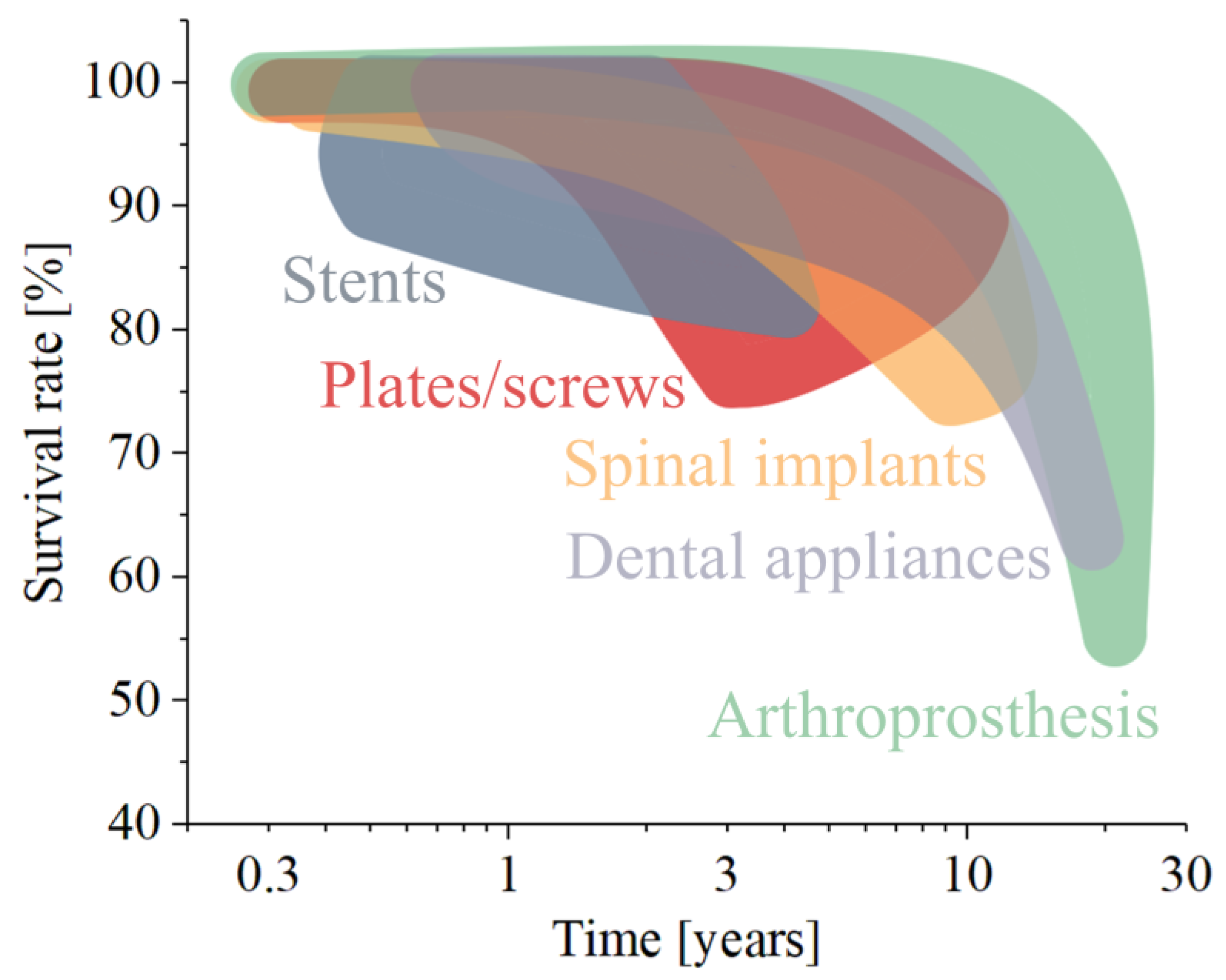{kind=link}
{kind=link}
Table 1.
Main titanium microstructural phases.
| Phase | Symbol | Structure | Description | References |
|---|---|---|---|---|
| Alpha | α | HCP | Allotropic form of titanium at low temperature | |
| Beta | β | BCC | Allotropic form of titanium at high temperature | [56] |
| Alpha2 | α2 | HCP | A compound, Ti3Al, which appears in a wide range of Al content | [57] |
| Gamma | γ | The intermetallic compound TiAl | [58] | |
| Alpha prime | α′ | HCP | Martensitic metastable structure | [59] |
| Alpha double prime | A″ | OR | Orthorhombic metastable martensitic structure | [60] |
| Beta prime or omega | β′ or ω | BCC | Metastable phases formed during quenching or aging | [61] |
Table 2.
List of the main titanium alloys that found application in the biological field, along with their most common microstructure, the specific applications that are commonly associated, and references to previous literature.
Table 2.
List of the main titanium alloys that found application in the biological field, along with their most common microstructure, the specific applications that are commonly associated, and references to previous literature.
| Alloy Name | Phase | Area of Application | References |
|---|---|---|---|
| CP-Ti (Grade 1) | α | Dental (uncommon) | [69,70] |
| CP-Ti (Grade 2) | α | Dental, Joint replacement | [71] |
| CP-Ti (Grade 3) | α | Dental | [72] |
| CP-Ti (Grade 4) | α | Joint replacement | [72] |
| Ti-8Al-1Mo-1V | α | - | [73] |
| Ti-6Al-2Nb-1Ta-0.8Mo | α | Joint replacement | [74,75] |
| Ti-6Al-2Zr-1Mo-1V | α | Joint replacement | [76] |
| Ti-6Al-4V (Grade 5) | α-β | Joint replacement, trauma, dental, spinal, etc. | [77] |
| Ti-6Al-4V ELI (Grade 23) | α-β | Joint replacement, trauma, cardiovascular, dental, spinal, etc. | [78] |
| Ti-6Al-7Nb | α-β | Joint replacement and dental | [79,80] |
| Ti-5Al-2.5Fe (Grade 9) | α-β | Dental | [81] |
| Ti3Al-2.5V | α-β | Joint replacement | [81] |
| Ti-6Al-6V-2Sn | α-β | Joint replacement | [82] |
| Ti-10Fe-10Ta-4Zr | α-β | Joint replacement | [83] |
| Ti-5Al-2Sn-2Zr-4Mo-4Cr | α-β | Joint replacement | [84] |
| Ti-4Al-4Mo-2Sn-0.5Si | α-β | Joint replacement | [85] |
| Ti-3Zr-2Sn-3Mo-25Nb | β | Joint replacement | [86] |
| Ti-13Nb-13Zr | β | Joint replacement and dental | [80] |
| Ti-12Mo-6Zr-2Fe | β | Joint replacement | [87,88,89] |
| Ti-15Mo | β | Joint replacement and dental | [90,91,92] |
| Ti-15Mo-5Zr-3Al | β | Joint replacement | [93,94] |
| Ti-15Mo-2.8Nb-0.2Si-0.260 | β | Joint replacement | [92,95,96] |
| Ti-16Nb-10Hf | β | Joint replacement | [97,98] |
| Ti-35.5Nb-7.3Zr-5.7Ta | β | Joint replacement | [99,100] |
| Ti-29Nb-13Ta-4.6Zr | β | Joint replacement | [101,102,103] |
| Ti-24Nb-4Zr-8Sn | β | Joint replacement | [104] |
| Ti-9Mn | β | Joint replacement | [105,106] |
| Ti-6Mn-4Mo | β | Joint replacement | [106] |
| Ti-10Fe-10Ta-4Zr | β | Joint replacement | [107,108] |
| Ti-12Cr | β | Joint replacement | [109] |
| Ti-11Cr-0.xO | β | Joint replacement | [110] |
| Ti-36Nb-2Ta-3Zr-0.3O | β | Joint replacement | [111] |
| Ti-24Nb-0.5O | β | Joint replacement | [112] |
| Ti-24Nb-0.5N | β | Joint replacement | [112] |
| Ti-23Nb-0.7Ta-2Zr | β | Joint replacement | [113] |
| Ti-23Nb-0.7Ta-2Zr-1.2O | β | Joint replacement | [113,114] |
| Ti-12Mo-6Zr-2Fe | β | Joint replacement | [115] |
| NiTi (Nitinol) | Cardiovascular, dental, joint replacement | [116] | |
| Ti-30Zr-xMo | Joint replacement | [117] |
Table 3.
Categories and biomedical applications for titanium alloys.
| Category | Uses | Alloys | Ref. |
|---|---|---|---|
| Dental implants | Braces, bridges, abutments, orthodontics, fixation devices | β-titanium, pure titanium, Ti-6Al-4V, Nitinol | [187,188,189,190,191,192,193,194,195,196,197,198,199,200,201,202,203,204,205,206,207,208,209,210,211,212,213,214,215,216,217,218,219,220,221] |
| Orthopedic implants | joint components (stems, cups, …), meshes, bone substitutes, fixation devices | Ti-6Al-4V, Ti-6Al-7Nb, Ti-15Mo, Ti-13Nb-13Zr, pure titanium, Nitinol | [222,223,224,225,226,227,228,229,230,231,232,233,234,235,236,237,238,239,240,241,242,243,244,245,246,247,248,249,250] |
| Trauma devices | Plates, screws, rods, nails | Ti-6Al-4V, Ti-6Al-7Nb, and pure titanium | [251,252,253,254,255,256,257,258,259,260,261] |
| Spinal implants | cages, discs, fixation devices | Ti-6Al-4V, pure titanium | [262,263,264,265,266,267,268,269,270,271] |
| Cardiovascular devices | Heart valves, catheters, guidewires, clips, stents, implantable defibrillators, ventricular assist devices | Nitinol, Ti-6Al-4V, Ti-6Al-7Nb, Ti-15Mo, pure titanium | [272,273,274,275,276,277,278,279,280,281,282,283,284,285,286,287,288,289,290,291,292] |
| Soft tissue implants | Fixation devices, hernia meshes, breast reconstruction meshes | Ti-6Al-4V, Ti-6Al-7Nb, pure titanium | [293,294,295,296] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Marin, E.; Lanzutti, A. Biomedical Applications of Titanium Alloys: A Comprehensive Review. Materials 2024, 17, 114. https://doi.org/10.3390/ma17010114
AMA Style
Marin E, Lanzutti A. Biomedical Applications of Titanium Alloys: A Comprehensive Review. Materials. 2024; 17(1):114. https://doi.org/10.3390/ma17010114
Chicago/Turabian StyleMarin, Elia, and Alex Lanzutti. 2024. "Biomedical Applications of Titanium Alloys: A Comprehensive Review" Materials 17, no. 1: 114. https://doi.org/10.3390/ma17010114
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.